

Personalised medicine in asthma: from curative to preventive medicine
- PMID: 28049124
- PMCID: PMC9489193
- DOI: 10.1183/16000617.0010-2016
Personalised medicine in asthma: from curative to preventive medicine
Abstract
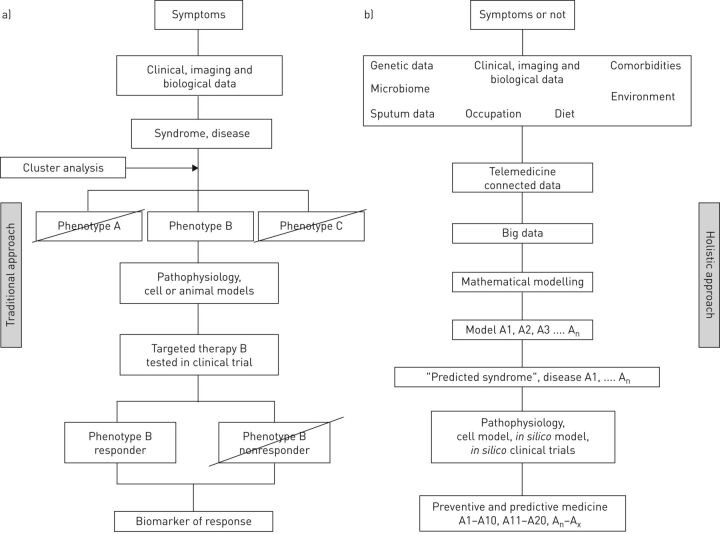
The concept of asthma has changed substantially in recent years. Asthma is now recognised as a heterogeneous entity that is complex to treat. The subdivision of asthma, provided by "cluster" analyses, has revealed various groups of asthma patients who share phenotypic features. These phenotypes underlie the need for personalised asthma therapy because, in contrast to the previous approach, treatment must be tailored to the individual patient. Determination of the patient's asthma phenotype is therefore essential but sometimes challenging, particularly in elderly patients with a multitude of comorbidities and a complex exposure history. This review first describes the various asthma phenotypes, some of which were defined empirically and others through cluster analysis, and then discusses personalisation of the patient's diagnosis and therapy, addressing in particular biological therapies and patient education. This personalised approach to curative medicine should make way in the coming years for personalised preventive and predictive medicine, focused on subjects at risk who are not yet ill, with the aim of preventing asthma before it occurs. The concept of personalised preventive medicine may seem a long way off, but is it really?
Copyright ©ERS 2017.
Conflict of interest statement
Conflict of interest: Disclosures can be found alongside this article at
Figures
References
-
- Wenzel SE, Schwartz LB, Langmack EL, et al. . Evidence that severe asthma can be divided pathologically into two inflammatory subtypes with distinct physiologic and clinical characteristics. Am J Respir Crit Care Med 1999; 160: 1001–1008. - PubMed
-
- Britton J. Symptoms and objective measures to define the asthma phenotype. Clin Exp Allergy 1998; 28: Suppl. 1, 2–7. - PubMed
-
- Wenzel SE. Asthma: defining of the persistent adult phenotypes. Lancet 2006; 368: 804–813. - PubMed
-
- Everitt BS, Landau S, Leese M. Cluster Analysis. London, Arnold, 2001.
-
- Hartigan JA. Clustering. Annu Rev Biophys Bioeng 1973; 2: 81–101. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical