

Validation of the Pediatric Index of Mortality 3 in a Single Pediatric Intensive Care Unit in Korea
- PMID: 28049251
- PMCID: PMC5220006
- DOI: 10.3346/jkms.2017.32.2.365
Validation of the Pediatric Index of Mortality 3 in a Single Pediatric Intensive Care Unit in Korea
Abstract
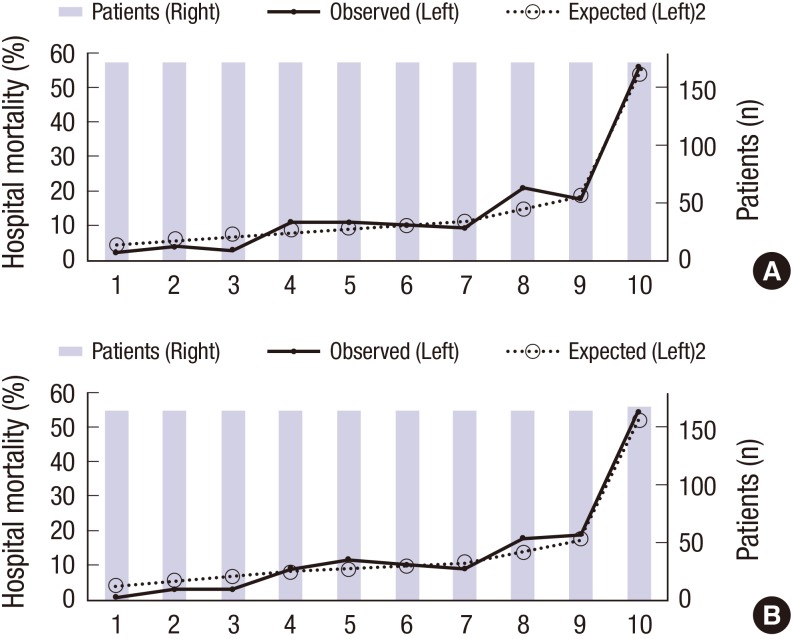
To compare mortality rate, the adjustment of case-mix variables is needed. The Pediatric Index of Mortality (PIM) 3 score is a widely used case-mix adjustment system of a pediatric intensive care unit (ICU), but there has been no validation study of it in Korea. We aim to validate the PIM3 in a Korean pediatric ICU, and extend the validation of the score from those aged 0-16 to 0-18 years, as patients aged 16-18 years are admitted to pediatric ICU in Korea. A retrospective cohort study of 1,710 patients was conducted in a tertiary pediatric ICU. To validate the score, the discriminatory power was assessed by calculating the area under the receiver-operating characteristic (ROC) curve, and calibration was evaluated by the Hosmer-Lemeshow goodness-of-fit (GOF) test. The observed mortality rate was 8.47%, and the predicted mortality rate was 6.57%. For patients aged < 18 years, the discrimination was acceptable (c-index = 0.76) and the calibration was good, with a χ² of 9.4 in the GOF test (P = 0.313). The observed mortality rate in the hemato-oncological subgroup was high (18.73%), as compared to the predicted mortality rate (7.13%), and the discrimination was unacceptable (c-index = 0.66). In conclusion, the PIM3 performed well in a Korean pediatric ICU. However, the application of the PIM3 to a hemato-oncological subgroup needs to be cautioned. Further studies on the performance of PIM3 in pediatric patients in adult ICUs and pediatric ICUs of primary and secondary hospitals are needed.
Keywords: Benchmarking; Child; Critical Care; Mortality; Risk Adjustment; Validation Study.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
Similar articles
-
Pediatric Index of Cardiac Surgical Intensive Care Mortality Risk Score for Pediatric Cardiac Critical Care.Pediatr Crit Care Med. 2015 Nov;16(9):846-52. doi: 10.1097/PCC.0000000000000489. Pediatr Crit Care Med. 2015. PMID: 26196254
-
Performance of PRISM (Pediatric Risk of Mortality) score and PIM (Pediatric Index of Mortality) score in a tertiary care pediatric ICU.Indian J Pediatr. 2010 Mar;77(3):267-71. doi: 10.1007/s12098-010-0031-3. Epub 2010 Feb 22. Indian J Pediatr. 2010. PMID: 20177831
-
Performance and analysis of four pediatric mortality prediction scores among critically ill children: A multicenter prospective observational study in four PICUs.Arch Pediatr. 2022 Aug;29(6):407-414. doi: 10.1016/j.arcped.2022.05.001. Epub 2022 Jun 14. Arch Pediatr. 2022. PMID: 35710758
-
Do interventions in an ICU affect the predictive ability of pediatric index of mortality and pediatric index of mortality-2 scores in a tertiary care hospital?Pediatr Crit Care Med. 2013 Feb;14(2):e70-6. doi: 10.1097/PCC.0b013e31827127cd. Pediatr Crit Care Med. 2013. PMID: 23287905
-
Scoring systems in pediatric intensive care: PRISM III versus PIM.Intensive Care Med. 2002 Feb;28(2):204-7. doi: 10.1007/s00134-001-1185-2. Epub 2002 Jan 12. Intensive Care Med. 2002. PMID: 11907665
Cited by
-
Are the Pediatric Index of Mortality 2 and 3 equal predictors of mortality? An intensive care unit-based concordance study.Rev Bras Ter Intensiva. 2020 Oct-Dec;32(4):578-584. doi: 10.5935/0103-507X.20200096. Rev Bras Ter Intensiva. 2020. PMID: 33470360 Free PMC article.
-
Internal validation and evaluation of the predictive performance of models based on the PRISM-3 (Pediatric Risk of Mortality) and PIM-3 (Pediatric Index of Mortality) scoring systems for predicting mortality in Pediatric Intensive Care Units (PICUs).BMC Pediatr. 2022 Apr 12;22(1):199. doi: 10.1186/s12887-022-03228-y. BMC Pediatr. 2022. PMID: 35413854 Free PMC article.
-
Multicenter validation of PIM3 and PIM2 in Brazilian pediatric intensive care units.Front Pediatr. 2022 Dec 14;10:1036007. doi: 10.3389/fped.2022.1036007. eCollection 2022. Front Pediatr. 2022. PMID: 36589158 Free PMC article.
-
Validation of Pediatric Index of Mortality 3 for Predicting Mortality among Patients Admitted to a Pediatric Intensive Care Unit.Acute Crit Care. 2018 Aug;33(3):170-177. doi: 10.4266/acc.2018.00150. Epub 2018 Aug 31. Acute Crit Care. 2018. PMID: 31723881 Free PMC article.
-
COVID-19 and Co-infection in Children: The Indian Perspectives.J Trop Pediatr. 2021 Aug 27;67(4):fmab073. doi: 10.1093/tropej/fmab073. J Trop Pediatr. 2021. PMID: 34478546 Free PMC article.
References
-
- Garland A. Improving the ICU: part 1. Chest. 2005;127:2151–2164. - PubMed
-
- Pollack MM, Alexander SR, Clarke N, Ruttimann UE, Tesselaar HM, Bachulis AC. Improved outcomes from tertiary center pediatric intensive care: a statewide comparison of tertiary and nontertiary care facilities. Crit Care Med. 1991;19:150–159. - PubMed
-
- Marcin JP, Pollack MM. Review of the methodologies and applications of scoring systems in neonatal and pediatric intensive care. Pediatr Crit Care Med. 2000;1:20–27. - PubMed
-
- Straney L, Clements A, Parslow RC, Pearson G, Shann F, Alexander J, Slater A, ANZICS Paediatric Study Group and the Paediatric Intensive Care Audit Network Paediatric index of mortality 3: an updated model for predicting mortality in pediatric intensive care*. Pediatr Crit Care Med. 2013;14:673–681. - PubMed
-
- Pollack MM, Patel KM, Ruttimann UE. PRISM III: an updated pediatric risk of mortality score. Crit Care Med. 1996;24:743–752. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
