

Perioperative changes in osteopontin and TGFβ1 plasma levels and their prognostic impact for radiotherapy in head and neck cancer
- PMID: 28049456
- PMCID: PMC5209814
- DOI: 10.1186/s12885-016-3024-4
Perioperative changes in osteopontin and TGFβ1 plasma levels and their prognostic impact for radiotherapy in head and neck cancer
Abstract
Background: In head and neck cancer little is known about the kinetics of osteopontin (OPN) expression after tumor resection. In this study we evaluated the time course of OPN plasma levels before and after surgery.
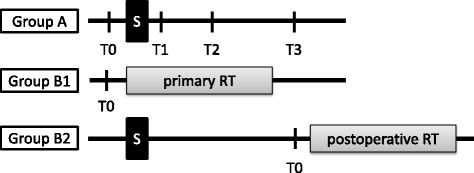
Methods: Between 2011 and 2013 41 consecutive head and neck cancer patients were enrolled in a prospective study (group A). At different time points plasma samples were collected: T0) before, T1) 1 day, T2) 1 week and T3) 4 weeks after surgery. Osteopontin and TGFβ1 plasma concentrations were measured with a commercial ELISA system. Data were compared to 131 head and neck cancer patients treated with primary (n = 42) or postoperative radiotherapy (n = 89; group B1 and B2).
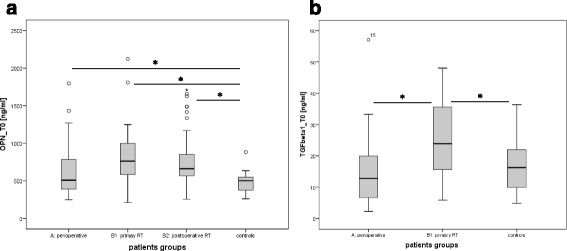
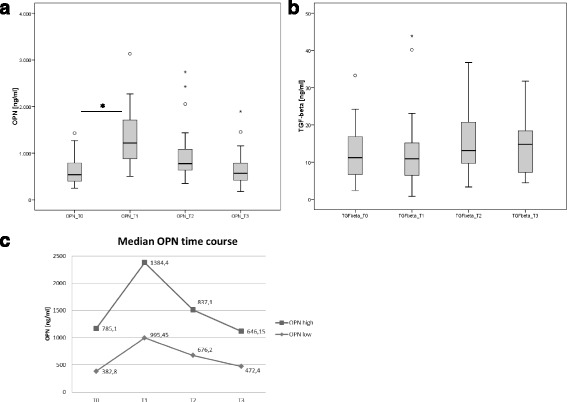
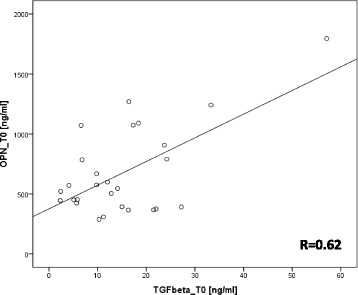
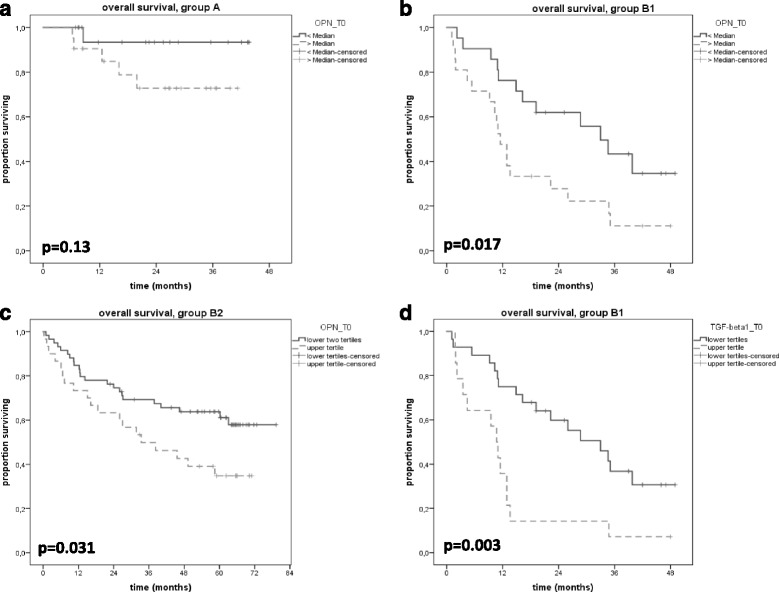
Results: A significant OPN increase was seen as early as 1 day after surgery (T0 to T1, p < 0.01). OPN levels decreased to base line 3-4 weeks after surgery. OPN values were correlated with postoperative TGFβ1 expression suggesting a relation to wound healing. Survival analysis showed a significant benefit for patients with lower OPN levels both in the primary and postoperative radiotherapy group (B1: 33 vs 11.5 months, p = 0.017, B2: median not reached vs 33.4, p = 0.031). TGFβ1 was also of prognostic significance in group B1 (33.0 vs 10.7 months, p = 0.003).
Conclusions: Patients with head and neck cancer showed an increase in osteopontin plasma levels directly after surgery. Four weeks later OPN concentration decreased to pre-surgery levels. This long lasting increase was presumably associated to wound healing. Both pretherapeutic osteopontin and TGFβ1 had prognostic impact.
Keywords: Head and neck cancer; Osteopontin; Perioperative changes; Survival; TGFβ1.
Figures
References
-
- Nguyen-Tan PF, Zhang Q, Ang KK, Weber RS, Rosenthal DI, Soulieres D, et al. Randomized phase III trial to test accelerated versus standard fractionation in combination with concurrent cisplatin for head and neck carcinomas in the Radiation Therapy Oncology Group 0129 trial: long-term report of efficacy and toxicity. J Clin Oncol. 2014;32:3858–66. doi: 10.1200/JCO.2014.55.3925. - DOI - PMC - PubMed
-
- Bourhis J, Sire C, Graff P, Gregoire V, Maingon P, Calais G, et al. Concomitant chemoradiotherapy versus acceleration of radiotherapy with or without concomitant chemotherapy in locally advanced head and neck carcinoma (GORTEC 99–02): an open-label phase 3 randomised trial. Lancet Oncol. 2012;13:145–53. doi: 10.1016/S1470-2045(11)70346-1. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
