

Expanding access to parasite-based malaria diagnosis through retail drug shops in Tanzania: evidence from a randomized trial and implications for treatment
- PMID: 28049481
- PMCID: PMC5209819
- DOI: 10.1186/s12936-016-1658-y
Expanding access to parasite-based malaria diagnosis through retail drug shops in Tanzania: evidence from a randomized trial and implications for treatment
Abstract
Background: Tanzania has seen a reduction in the fraction of fevers caused by malaria, likely due in part to scale-up of control measures. While national guidelines require parasite-based diagnosis prior to treatment, it is estimated that more than half of suspected malaria treatment-seeking in Tanzania initiates in the private retail sector, where diagnosis by malaria rapid diagnostic test (RDT) or microscopy is illegal. This pilot study investigated whether the introduction of RDTs into Accredited Drug Dispensing Outlets (ADDOs) under realistic market conditions would improve case management practices.
Methods: Dispensers from ADDOs in two intervention districts in Tanzania were trained to stock and perform RDTs and monitored quarterly. Each district was assigned a different recommended retail price to evaluate the need for a subsidy. Malaria RDT and artemisinin-based combination therapy (ACT) uptake and availability were measured pre-intervention and 1 year post-intervention through structured surveys of ADDO owners and exiting customers in both intervention districts and one contiguous control district. Descriptive analysis and logistic regression were used to compare the three districts and identify predictive variables for testing.
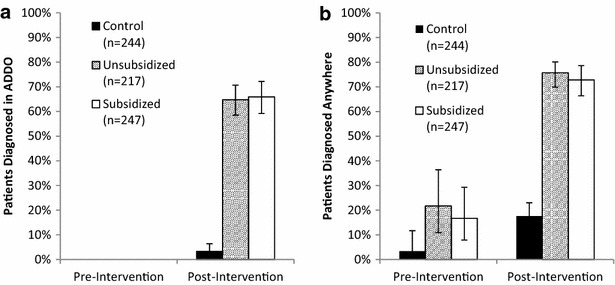
Results and discussion: A total of 310 dispensers from 262 ADDOs were trained to stock and perform RDTs. RDT availability in intervention ADDOs increased from 1% (n = 172) to 73% (n = 163) during the study; ACT medicines were available in 75% of 260 pre-intervention and 68% of 254 post-intervention ADDOs. Pre-treatment testing performed within the ADDO increased from 0 to 65% of suspected malaria patients who visited a shop (95% CI 60.8-69.6%) with no difference between intervention districts. Overall parasite-based diagnosis increased from 19 to 74% in intervention districts and from 3 to 18% in the control district. Prior knowledge of RDT availability (aOR = 1.9, p = 0.03) and RDT experience (aOR = 1.9, p = 0.01) were predictors for testing. Adherence data indicated that 75% of malaria positives received ACT, while 3% of negatives received ACT.
Conclusions: Trained and supervised ADDO dispensers in rural Tanzania performed and sold RDTs under real market conditions to two-thirds of suspected malaria patients during this one-year pilot. These results support the hypothesis that introducing RDTs into regulated private retail sector settings can improve malaria testing and treatment practices without an RDT subsidy. Trial registration ISRCTN ISRCTN14115509.
Keywords: Parasite-based malaria diagnosis; Private retail sector; Rapid diagnostic test; Tanzania.
Figures


References
-
- Tanzania Commission for AIDS (TACAIDS), Zanzibar AIDS Commission (ZAC), National Bureau of Statistics (NBS), Office of Chief Government Statistician (OCGS), and Macro International Inc. Tanzania HIV/AIDS and Malaria Indicator Survey 2007–2008. 2008. http://dhsprogram.com/pubs/pdf/AIS6/AIS6_05_14_09.pdf. Accessed 2 Feb 2016.
-
- Tanzania Commission for AIDS (TACAIDS), Zanzibar AIDS Commission (ZAC), National Bureau of Statistics (NBS), Office of Chief Government Statistician (OCGS), and ICF International. Tanzania HIV/AIDS and Malaria Indicator Survey 2011–2012. 2013. http://dhsprogram.com/pubs/pdf/AIS11/AIS11.pdf. Accessed 2 Feb 2016.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
