

Effects of a mutual recovery intervention on mental health in depressed elderly community-dwelling adults: a pilot study
- PMID: 28049503
- PMCID: PMC5209883
- DOI: 10.1186/s12889-016-3930-z
Effects of a mutual recovery intervention on mental health in depressed elderly community-dwelling adults: a pilot study
Abstract
Background: The prevalence of depression in the elderly is growing worldwide, and the population aging in China makes depression a major health problem for the elderly adults and a tremendous burden to the society. Effective interventions should be determined to provide an approach solving the problem and improving the situation. This study examined the effectiveness of a mutual recovery program intervention on depressive symptom, sleep quality, and well-being in community-dwelling elderly adults with depressive symptom in Shanghai.
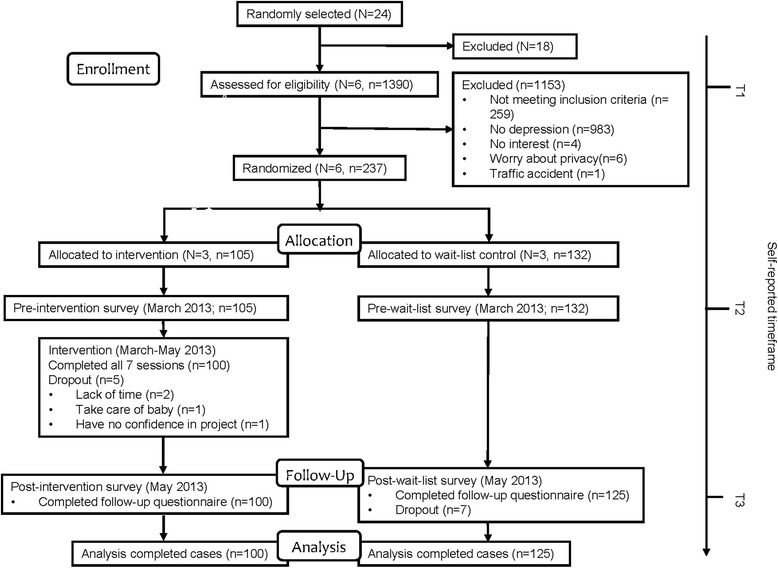
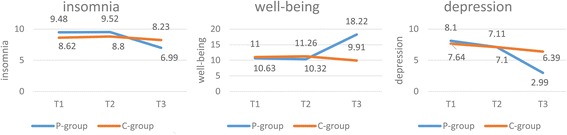
Methods: Recruitment was performed between July 2012 and August 2012. Using a cluster randomized wait-list controlled design, we randomized 6 communities (n = 237) into either the intervention group (3 communities, n = 105) or to a wait-list control group (3 communities, n = 132). All participants met the inclusion criteria for depression, which were defined by The Geriatric Depression Scale (GDS-15). From March to May of 2013, participants in the intervention group underwent a 2-month mutual recovery program intervention. The intervention included seven 90-min, weekly sessions that were based on a standardized self-designed schedule. Depression was used as primary outcome at three measurement moments: baseline (T1), before intervention at 24 weeks (T2), and immediately after intervention at 32 weeks (T3). Well-being and sleep quality were used as the secondary outcomes, and were evaluated based on the WHO-5 Well-being Index (WHO-5) and the Self-administered Sleep Questionnaire (SSQ). Finally, a total of 225 participants who completed all the sessions and the three measurements entered the final analysis. Mixed-model repeated measures ANOVAs were performed to estimate the intervention effects.
Results: There was no significant difference in gender, marriage, age structure, post-work type, and education background between the intervention and control group at baseline. Multivariate ANOVAs showed that there was no significant difference within the groups in terms of sleep, well-being, and depression at baseline and before the intervention. Mixed-model repeated measures ANOVAs detected a group × time interaction on depression, sleep, and well-being and showed a favorable intervention effect within groups immediately after the intervention.
Conclusions: The mutual recovery program could be a creative and effective approach to improve mental health in older community-dwelling adults with depressive symptom.
Keywords: Depression; Elderly population; Intervention; Mental health; Well-being.
Figures
Similar articles
-
Effects of exercise and horticultural intervention on the brain and mental health in older adults with depressive symptoms and memory problems: study protocol for a randomized controlled trial [UMIN000018547].Trials. 2015 Nov 4;16:499. doi: 10.1186/s13063-015-1032-3. Trials. 2015. PMID: 26537979 Free PMC article. Clinical Trial.
-
Novel Augmentation Strategies in Major Depression.Dan Med J. 2017 Apr;64(4):B5338. Dan Med J. 2017. PMID: 28385173 Review.
-
Physical fitness exercise versus cognitive behavior therapy on reducing the depressive symptoms among community-dwelling elderly adults: A randomized controlled trial.Int J Nurs Stud. 2015 Oct;52(10):1542-52. doi: 10.1016/j.ijnurstu.2015.05.013. Epub 2015 Jun 10. Int J Nurs Stud. 2015. PMID: 26105535 Clinical Trial.
-
The Happy Older Latinos are Active (HOLA) health promotion and prevention study: study protocol for a pilot randomized controlled trial.Trials. 2015 Dec 18;16:579. doi: 10.1186/s13063-015-1113-3. Trials. 2015. PMID: 26683695 Free PMC article. Clinical Trial.
-
[Epidemiological study of sleep disorder in the elderly].Zhonghua Liu Xing Bing Xue Za Zhi. 2017 Jul 10;38(7):988-992. doi: 10.3760/cma.j.issn.0254-6450.2017.07.028. Zhonghua Liu Xing Bing Xue Za Zhi. 2017. PMID: 28738480 Review. Chinese.
Cited by
-
A study of the effects of dance/movement therapy on parenting stress and emotions in mothers of children with autism spectrum disorder.Front Psychiatry. 2025 Mar 7;16:1465677. doi: 10.3389/fpsyt.2025.1465677. eCollection 2025. Front Psychiatry. 2025. PMID: 40123600 Free PMC article.
-
Efficacy of Psychological Interventions Towards the Reduction of High-Risk Sexual Behaviors Among People Living with HIV: A Systematic Review and Meta-analysis, 2010-2020.AIDS Behav. 2021 Oct;25(10):3355-3376. doi: 10.1007/s10461-021-03181-4. Epub 2021 Feb 8. AIDS Behav. 2021. PMID: 33559070 Free PMC article.
-
Rasch analysis of the hospital anxiety and depression scale among Chinese cataract patients.PLoS One. 2017 Sep 26;12(9):e0185287. doi: 10.1371/journal.pone.0185287. eCollection 2017. PLoS One. 2017. PMID: 28949992 Free PMC article.
-
Family function, coping style and well-being affect job burnout among telecommunication employees: a cross-sectional study in China.Front Public Health. 2025 May 21;13:1567123. doi: 10.3389/fpubh.2025.1567123. eCollection 2025. Front Public Health. 2025. PMID: 40469606 Free PMC article.
-
A systematic review and meta-analysis of psychological interventions to improve mental wellbeing.Nat Hum Behav. 2021 May;5(5):631-652. doi: 10.1038/s41562-021-01093-w. Epub 2021 Apr 19. Nat Hum Behav. 2021. PMID: 33875837
References
-
- Yu Y, Tao L, Yang G. China’s ageing population and the need of the public health service. Chin J Gerontol. 2013;33(01):220–222.
-
- Liu S, Zhang R, Zhang X, Sun L. The situation of China’s ageing population and health care. Prac J Med Pharm. 2013;30(01):91–92.
-
- Hu S. Social economical burden of depressive disorders and its countermeasures. Chin J of Prev Med. 2005;39(04):283–284.
-
- Wang S, Yang X, Zhu X. Depressive disorders among elderly and related issues. Chin J Misdiagnostics. 2001;01(09):1372–1374.
-
- Charney DS, Reynolds CR, Lewis L, Lebowitz BD, Sunderland T, Alexopoulos GS, Blazer DG, Katz IR, Meyers BS, Arean PA, et al. Depression and Bipolar Support Alliance consensus statement on the unmet needs in diagnosis and treatment of mood disorders in late life. Arch Gen Psychiatry. 2003;60(7):664–672. doi: 10.1001/archpsyc.60.7.664. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
