

Incidence and admission rates for severe malaria and their impact on mortality in Africa
- PMID: 28049519
- PMCID: PMC5209951
- DOI: 10.1186/s12936-016-1650-6
Incidence and admission rates for severe malaria and their impact on mortality in Africa
Abstract
Background: Appropriate treatment of life-threatening Plasmodium falciparum malaria requires in-patient care. Although the proportion of severe cases accessing in-patient care in endemic settings strongly affects overall case fatality rates and thus disease burden, this proportion is generally unknown. At present, estimates of malaria mortality are driven by prevalence or overall clinical incidence data, ignoring differences in case fatality resulting from variations in access. Consequently, the overall impact of preventive interventions on disease burden have not been validly compared with those of improvements in access to case management or its quality.
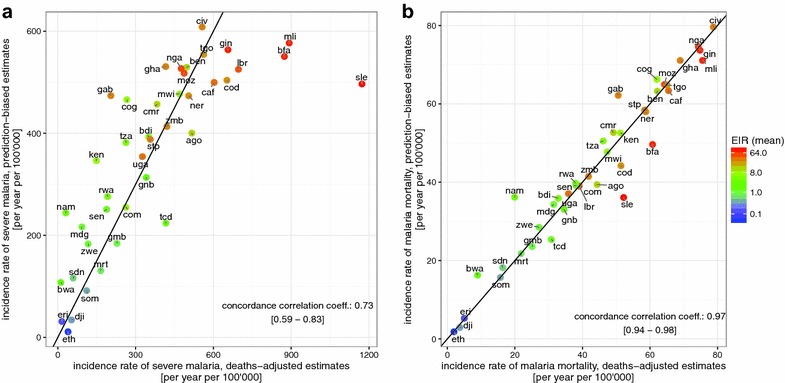
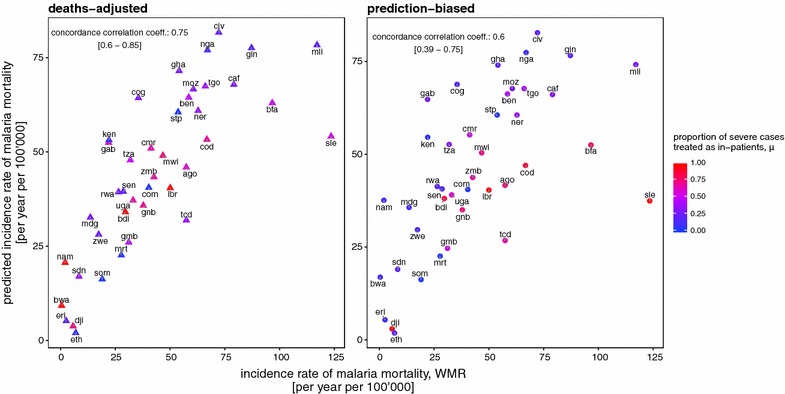
Methods: Using a simulation-based approach, severe malaria admission rates and the subsequent severe malaria disease and mortality rates for 41 malaria endemic countries of sub-Saharan Africa were estimated. Country differences in transmission and health care settings were captured by use of high spatial resolution data on demographics and falciparum malaria prevalence, as well as national level estimates of effective coverage of treatment for uncomplicated malaria. Reported and modelled estimates of cases, admissions and malaria deaths from the World Malaria Report, along with predicted burden from simulations, were combined to provide revised estimates of access to in-patient care and case fatality rates.
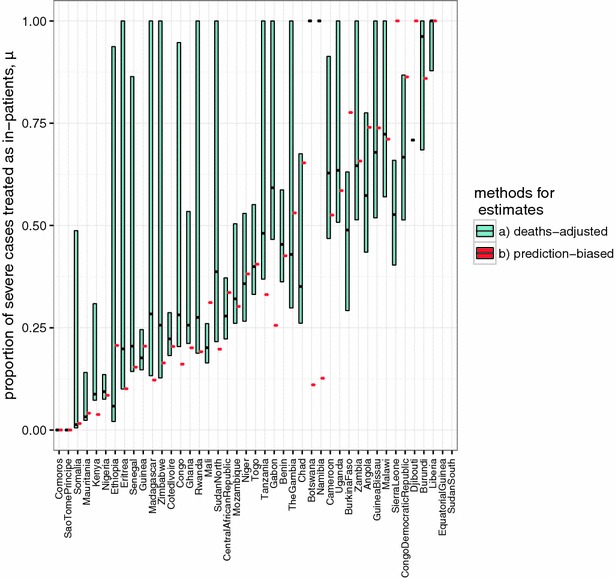
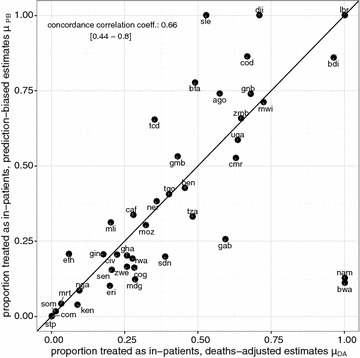
Results: There is substantial variation between countries' in-patient admission rates and estimated levels of case fatality rates. It was found that for many African countries, most patients admitted for in-patient treatment would not meet strict criteria for severe disease and that for some countries only a small proportion of the total severe cases are admitted. Estimates are highly sensitive to the assumed community case fatality rates. Re-estimation of national level malaria mortality rates suggests that there is substantial burden attributable to inefficient in-patient access and treatment of severe disease.
Conclusions: The model-based methods proposed here offer a standardized approach to estimate the numbers of severe malaria cases and deaths based on national level reporting, allowing for coverage of both curative and preventive interventions. This makes possible direct comparisons of the potential benefits of scaling-up either category of interventions. The profound uncertainties around these estimates highlight the need for better data.
Figures
References
-
- Thwing J, Eisele TP, Steketee RW. Protective efficacy of malaria case management and intermittent preventive treatment for preventing malaria mortality in children: a systematic review for the Lives Saved Tool. BMC Public Health. 2011;11(Suppl 3):S14. doi: 10.1186/1471-2458-11-S3-S14. - DOI - PMC - PubMed
-
- WHO . World malaria report 2015. Geneva: World Health Organization; 2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
