

The Hematologic Definition of Monoclonal Gammopathy of Undetermined Significance in Relation to Paraproteinemic Keratopathy (An American Ophthalmological Society Thesis)
- PMID: 28050052
- PMCID: PMC5189924
The Hematologic Definition of Monoclonal Gammopathy of Undetermined Significance in Relation to Paraproteinemic Keratopathy (An American Ophthalmological Society Thesis)
Erratum in
-
Erratum: The Hematologic Definition of Monoclonal Gammopathy of Undetermined Significance in Relation to Paraproteinemic Keratopathy (An American Ophthalmological Society Thesis).Trans Am Ophthalmol Soc. 2016 Aug;114:T7C1. Trans Am Ophthalmol Soc. 2016. PMID: 28260821 Free PMC article.
Abstract
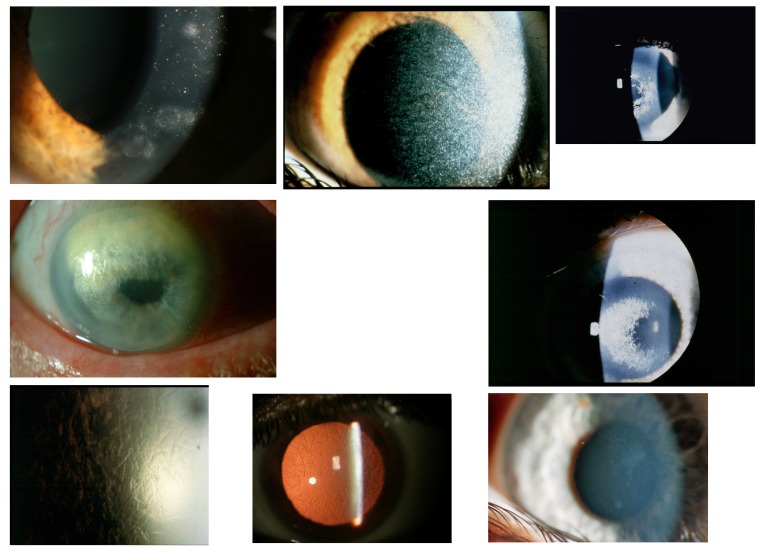
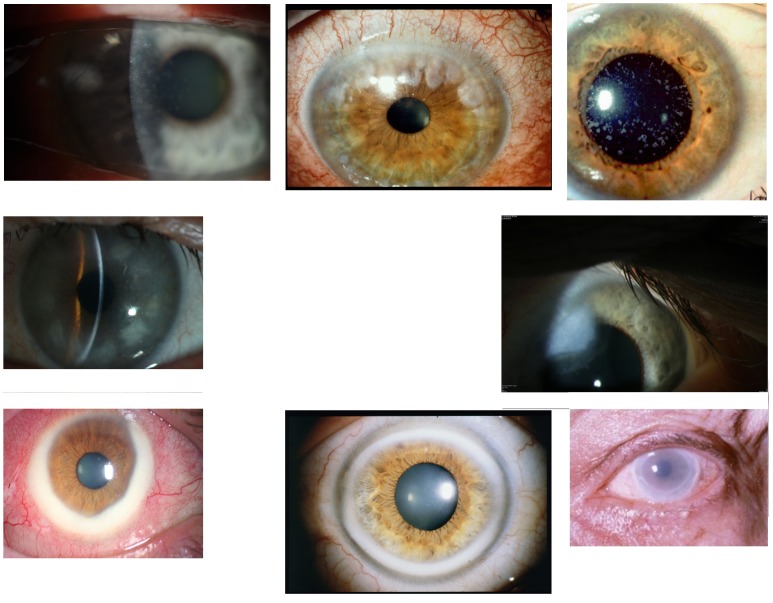
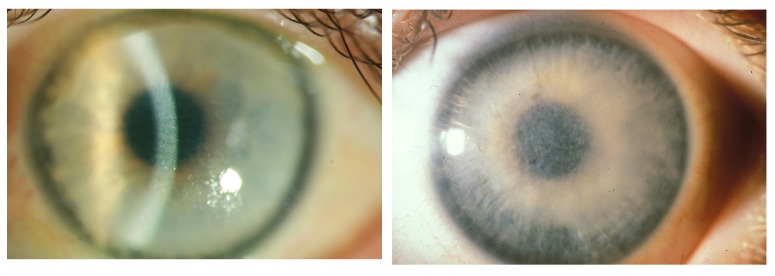
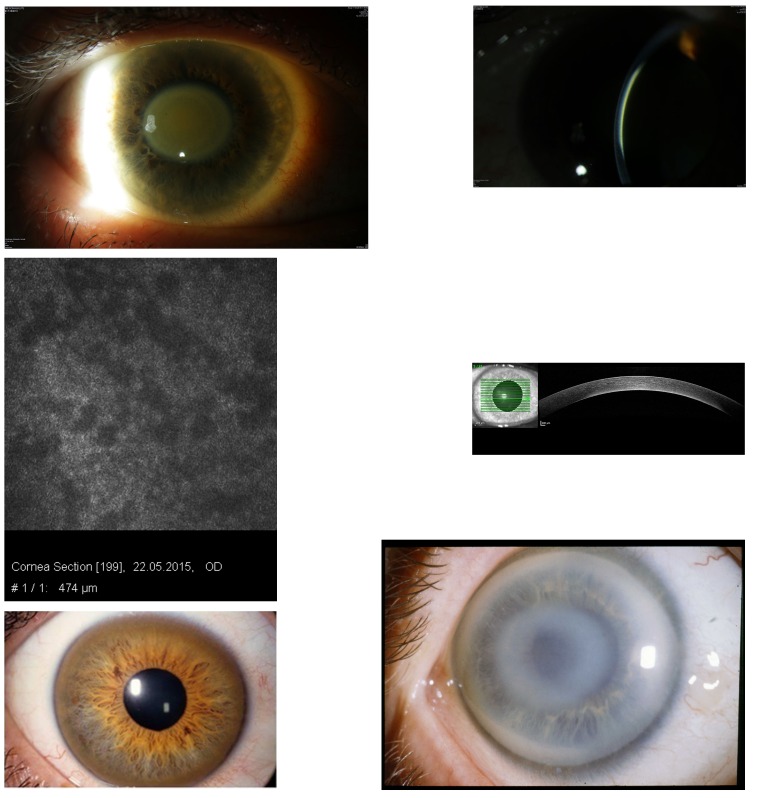
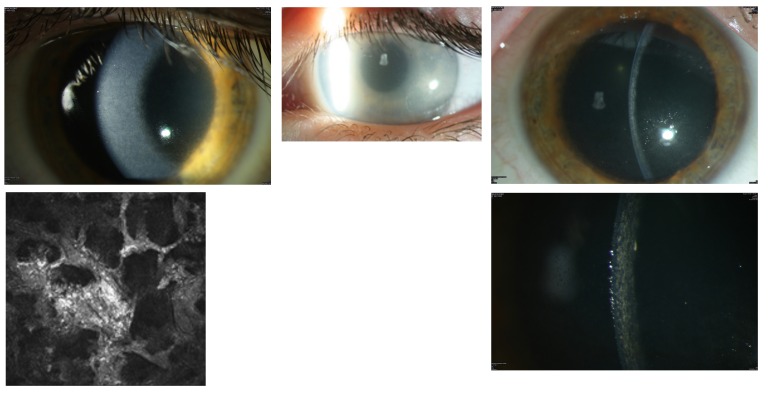
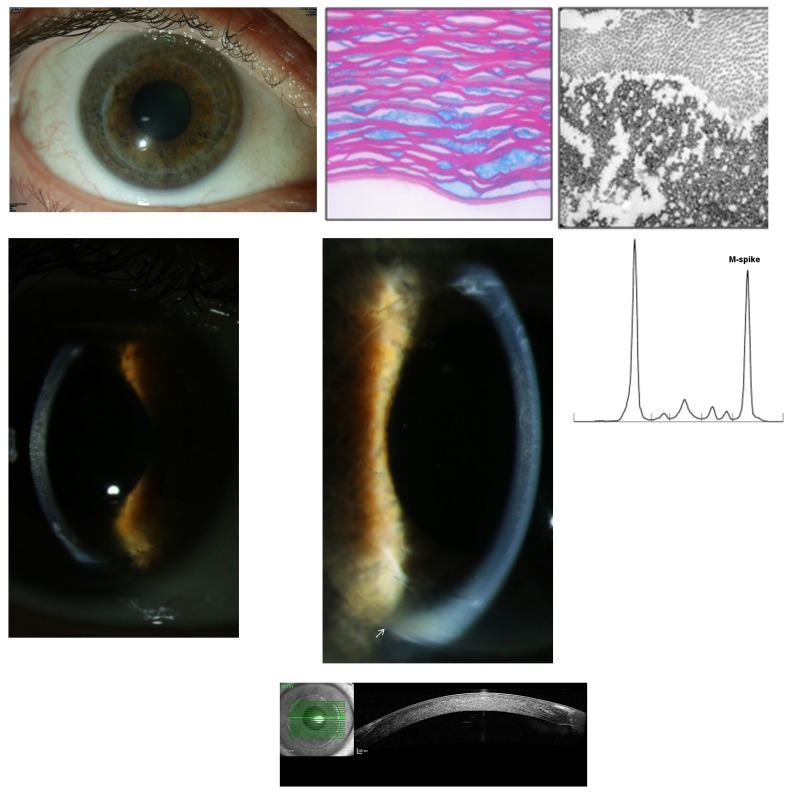
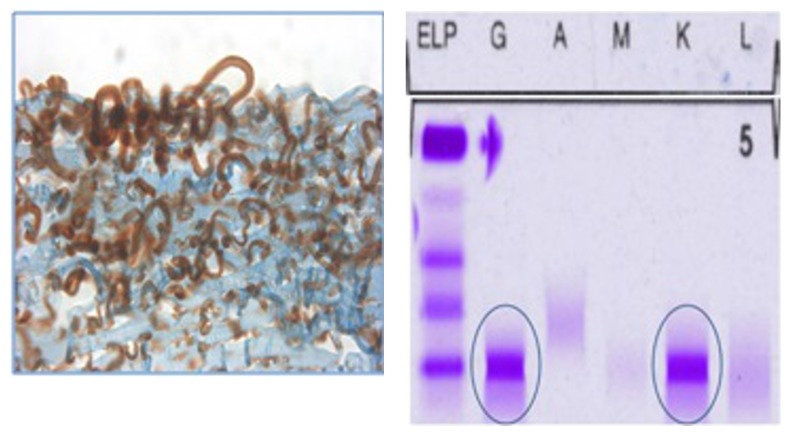
Purpose: To determine if paraproteinemic keratopathy (PPK) in the setting of monoclonal gammopathy of undetermined significance (MGUS) causes distinct patterns of corneal opacification that can be distinguished from hereditary, immunologic, or inflammatory causes.
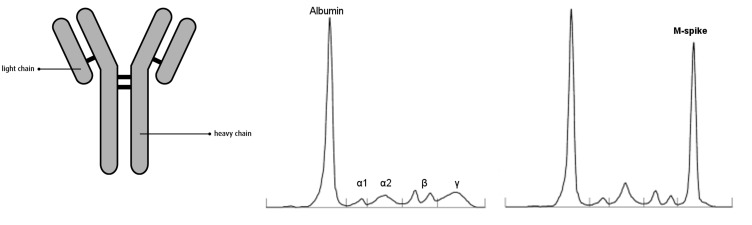
Methods: A retrospective, interventional study of patients showed distinct bilateral opacity patterns of the cornea at the eye clinics of Hanau, Mainz, Helsinki, Marburg, and Berlin between 1993 and 2015. Data on patient characteristics and clinical features on ophthalmic examination were collected, and serum protein profiles were evaluated. A literature review and analysis of all published studies of MGUS with PPK is also presented.
Results: The largest group of patients diagnosed with MGUS-induced PPK is analyzed in this study. We studied 22 eyes of 11 patients (6 male, aged 43 to 65, mean age 54; 5 female, aged 49 to 76, mean age 61) with distinct corneal opacities and visual impairment who were first suspected of having hereditary, inflammatory, or immunologic corneal entities. Subsequently, serum protein electrophoresis revealed MGUS to be the cause of the PPK. Literature review revealed 72 patients with bilateral PPK (34 male, mean age 57; 38 female, mean age 58) in 51 studies of MGUS published from 1934 to 2015 and disclosed six additional corneal opacity patterns.
Conclusions: This thesis shows that MGUS is not always an asymptomatic disorder, in contrast to the hematologic definition, which has no hint of PPK. The MGUS-induced PPK can mimic many other diseases of the anterior layer of the eye. A new clinical classification for PPK in MGUS is proposed.
Figures
References
-
- Crawford J, Eye MK, Cohen HJ. Evaluation of monoclonal gammopathies in the “well” elderly. Am J Med. 1987;82(1):39–45. - PubMed
-
- O’Connell TX, Horita TJ, Kasravi B. Understanding and interpreting serum protein electrophoresis. Am Fam Physician. 2005;71(1):105–112. - PubMed
-
- Allansmith MR, McClellan BH. Immunoglobulins in the human cornea. Am J Ophthalmol. 1975;80(1):123–132. - PubMed
-
- Bourne WM, Kyle RA, Brubaker RF, Greip PR. Incidence of corneal crystals in the monoclonal gammopathies. Am J Ophthalmol. 1989;107(2):192–193. - PubMed
-
- Steuhl K-P, Knorr M, Rohrbach JM, Lisch W, Kaiserling E, Thiel H-J. Paraproteinemic corneal deposits in plasma cell myeloma. Am J Ophthalmol. 1991;111(3):312–318. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
