

Bacillus cereus bacteraemia: comparison between haematologic and nonhaematologic patients
- PMID: 28050250
- PMCID: PMC5192042
- DOI: 10.1016/j.nmni.2016.11.011
Bacillus cereus bacteraemia: comparison between haematologic and nonhaematologic patients
Abstract
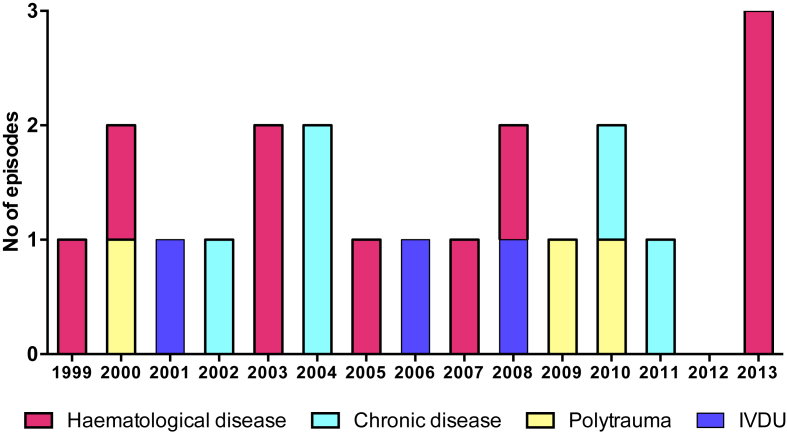
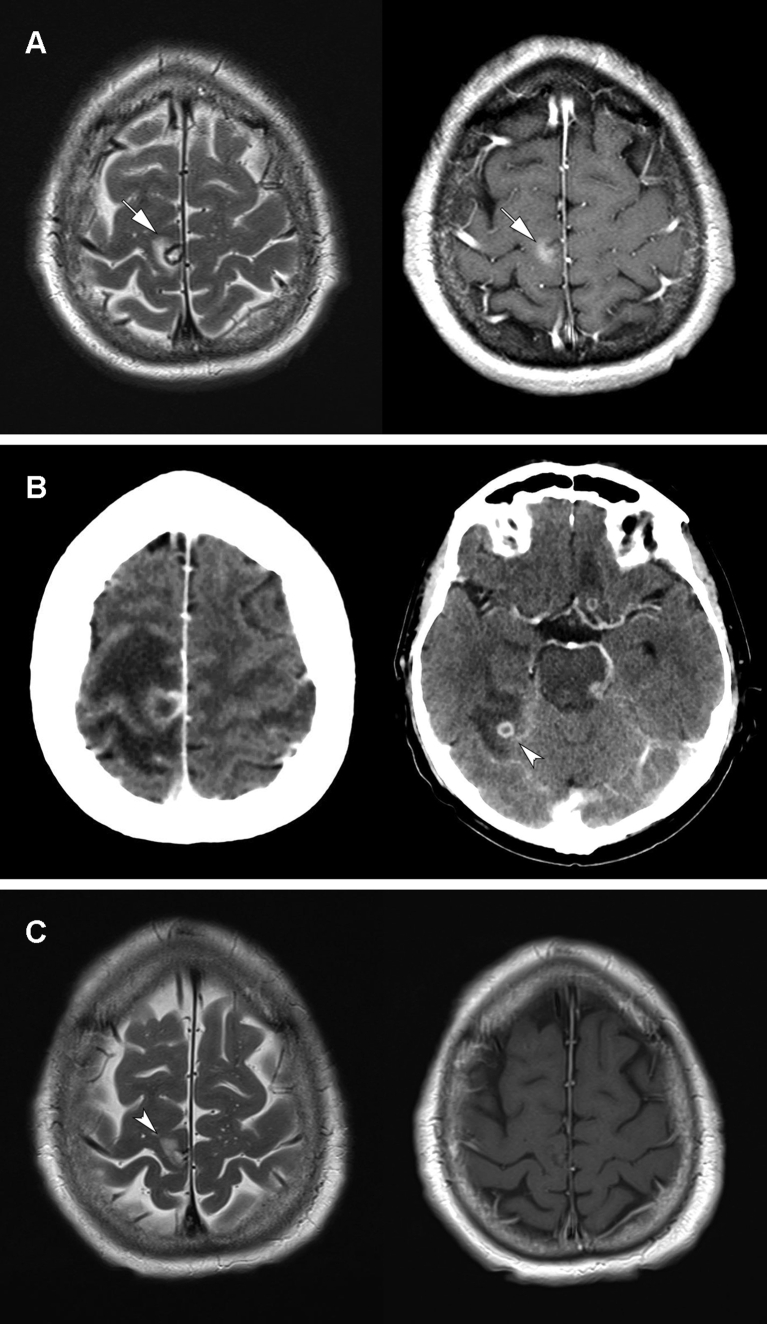
Bacillus cereus bacteraemia can be severe, especially among patients with haematologic malignancy. We retrospectively reviewed first episodes of true B. cereus bacteraemia (more than one positive bottle plus signs of infection) at our institution between 1997 and 2013 with the aim to compare haematologic versus nonhaematologic patients and analyse episodes with complicated outcome. Among 56 episodes of positive-blood cultures for B. cereus, 21 were considered significant. Median age was 54 years (range 23-82 years). Ten patients (48%) had a haematologic malignancy; all were neutropenic at the time of B. cereus bacteraemia. Nonhaematologic patients were either intravenous drug users (n = 3, 14%), polytraumatized (n = 3, 14%) or had multiple chronic comorbidities (n = 5, 24%). Most episodes were hospital acquired (15, 71%). Sources of bacteraemia were intravascular catheter (n = 11, 52%), digestive tract (n = 6, 29%), drug injection (n = 3, 14%) and wound (n = 1, 5%). Adequate antibiotic therapy was provided to 18 patients (86%) during a median of 17 days (range 2-253 days). The intravascular catheter was removed in eight cases (42%). Three haematologic patients had a complicated course with neurologic complications (meningoencephalitis and cerebral abscesses). Complications appeared to be associated with catheter infection (100% of complicated cases vs. 29% of noncomplicated cases). In conclusion, B. cereus bacteraemia can have a complicated course in a subset of patients, mainly those with haematologic malignancy. Catheter infection may be associated with a worse outcome with frequent neurologic complications.
Keywords: Bacillus cereus; bacteraemia; central nervous system; intravascular catheter; neutropenia.
Figures
References
-
- Dubouix A., Bonnet E., Alvarez M., Bensafi H., Archambaud M., Chaminade B. Bacillus cereus infections in traumatology–orthopaedics department: retrospective investigation and improvement of healthcare practices. J Infect. 2005;50:22–30. - PubMed
-
- Kotiranta A., Lounatmaa K., Haapasalo M. Epidemiology and pathogenesis of Bacillus cereus infections. Microbes Infect. 2000;2:189–198. - PubMed
-
- Tuazon C.U., Murray H.W., Levy C., Solny M.N., Curtin J.A., Sheagren J.N. Serious infections from Bacillus sp. JAMA. 1979;241:1137–1140. - PubMed
-
- Inoue D., Nagai Y., Mori M., Nagano S., Takiuchi Y., Arima H. Fulminant sepsis caused by Bacillus cereus in patients with hematologic malignancies: analysis of its prognosis and risk factors. Leuk Lymphoma. 2010;51:860–869. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources