

What is the Accuracy of Nuclear Imaging in the Assessment of Periprosthetic Knee Infection? A Meta-analysis
- PMID: 28050818
- PMCID: PMC5384926
- DOI: 10.1007/s11999-016-5218-0
What is the Accuracy of Nuclear Imaging in the Assessment of Periprosthetic Knee Infection? A Meta-analysis
Erratum in
-
Erratum to: What is the Accuracy of Nuclear Imaging in the Assessment of Periprosthetic Knee Infection? A Meta-analysis.Clin Orthop Relat Res. 2017 Jun;475(6):1753-1754. doi: 10.1007/s11999-017-5327-4. Clin Orthop Relat Res. 2017. PMID: 28374347 Free PMC article. No abstract available.
Abstract
Background: In the assessment of possible periprosthetic knee infection, various imaging modalities are used without consensus regarding the most accurate technique.
Questions/purposes: To perform a meta-analysis to compare the accuracy of various applied imaging modalities in the assessment of periprosthetic knee infection.
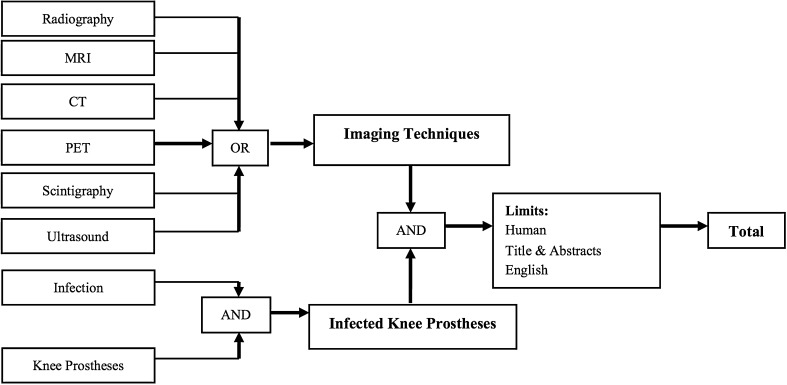
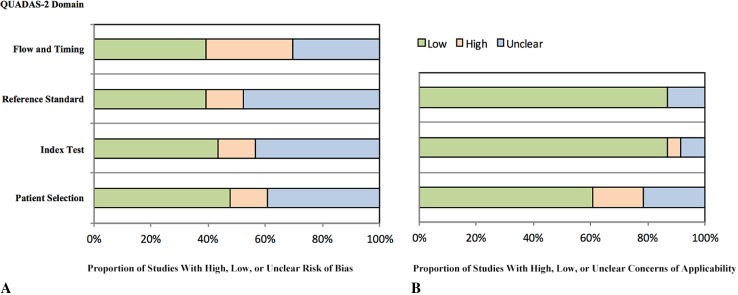
Methods: A systematic review and meta-analysis was conducted with a comprehensive search of MEDLINE and Embase® in accordance with the PRISMA and Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) recommendations to identify clinical studies in which periprosthetic knee infection was investigated with different imaging modalities. The sensitivity and specificity of each imaging technique were determined and compared with the results of microbiologic and histologic analyses, intraoperative findings, and clinical followup of more than 6 months. A total of 23 studies, published between 1990 and 2015, were included for meta-analysis, representing 1027 diagnostic images of symptomatic knee prostheses. Quality of the included studies showed low concerns regarding external validity, whereas internal validity indicated more concerns regarding the risk of bias. The most important concerns were found in the lack of uniform criteria for the diagnosis of a periprosthetic infection and the flow and timing of the included studies. Differences among techniques were tested at a probability less than 0.05 level. Where there was slight overlap of confidence intervals for two means, it is possible for the point estimates to be statistically different from one another at a probability less than 0.05. The z-test was used to statistically analyze differences in these situations.
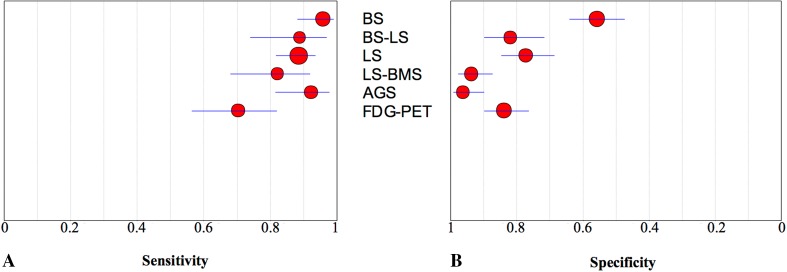
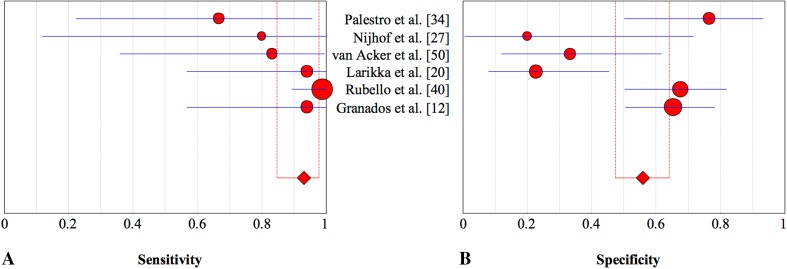
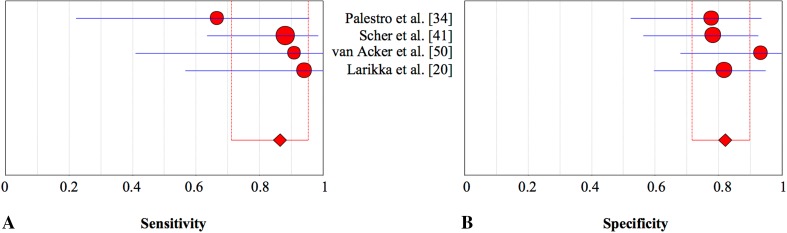
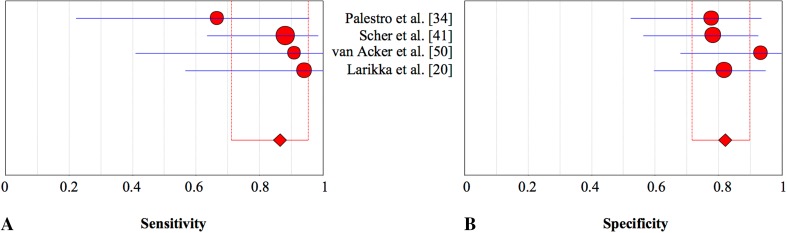
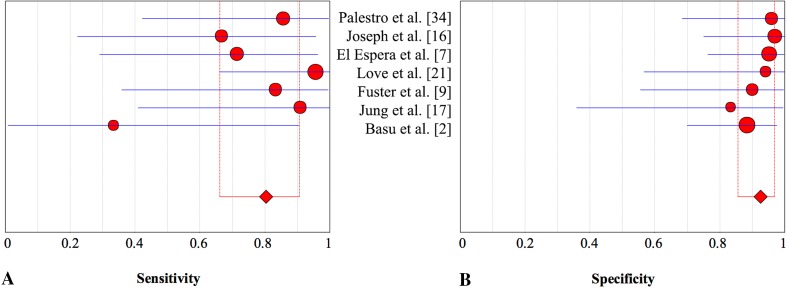
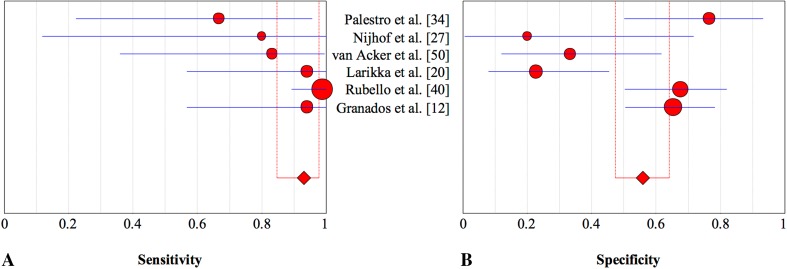
Results: Bone scintigraphy was less specific than all other modalities tested (56%; 95% CI, 0.47-0.64; p < 0.001), and leukocyte scintigraphy (77%; 95% CI, 0.69-0.85) was less specific than antigranulocyte scintigraphy (95%; 95% CI, 0.88-0.98; p < 0.001) or combined leukocyte and bone marrow scintigraphy (93%; 95% CI, 0.86-0.97; p < 0.001). Fluorodeoxyglucose positron emission tomography (FDG-PET) (84%; 95% CI, 0.76-0.90) was more specific than bone scintigraphy (56%; 95% CI, 0.47-0.64; p < 0.001), and less specific than antigranulocyte scintigraphy (95%; 95% CI, 0.88-0.98; p = 0.02) and combined leukocyte and bone marrow scintigraphy (93%; 95% CI, 0.86-0.97; p < 0.001). Leukocyte scintigraphy (88%; 95% CI, 0.81-0.93; p = 0.01) and antigranulocyte scintigraphy (90%; 95% CI, 0.78-0.96; p = 0.02) were more sensitive than FGD-PET (70%; 95% CI, 0.56-0.81). However, because of broad overlapping of confidence intervals, no differences in sensitivity were observed among the other modalities, including combined bone scintigraphy (93%; 95% CI, 0.85-0.98) or combined leukocyte and bone marrow scintigraphy (80%; 95% CI, 0.66-0.91; p > 0.05 for all paired comparisons).
Conclusions: Based on current evidence, antigranulocyte scintigraphy and combined leukocyte and bone marrow scintigraphy appear to be highly specific imaging modalities in confirming periprosthetic knee infection. Bone scintigraphy was a highly sensitive imaging technique but lacks the specificity needed to differentiate among various conditions that cause painful knee prostheses. FDG-PET may not be the preferred imaging modality because it is more expensive and not more effective in confirming periprosthetic knee infection.
Level of evidence: Level III, diagnostic study.
Figures
Comment in
-
CORR Insights®: What is the Accuracy of Nuclear Imaging in the Assessment of Periprosthetic Knee Infection? A Meta-analysis.Clin Orthop Relat Res. 2017 May;475(5):1411-1413. doi: 10.1007/s11999-017-5265-1. Epub 2017 Feb 2. Clin Orthop Relat Res. 2017. PMID: 28155210 Free PMC article. No abstract available.
References
-
- Basu S, Kwee TC, Saboury B, Garino JP, Nelson CL, Zhuang H, Parsons M, Chen W, Kumar R, Salavati A, Werner TJ, Alavi A. FDG PET for diagnosing infection in hip and knee prostheses: prospective study in 221 prostheses and subgroup comparison with combined (111)In-labeled leukocyte/(99 m)Tc-sulfur colloid bone marrow imaging in 88 prostheses. Clin Nucl Med. 2014;39:609–615. doi: 10.1097/RLU.0000000000000464. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
