

Pulsatile gonadotropin-releasing hormone therapy is associated with earlier spermatogenesis compared to combined gonadotropin therapy in patients with congenital hypogonadotropic hypogonadism
- PMID: 28051040
- PMCID: PMC5676428
- DOI: 10.4103/1008-682X.193568
Pulsatile gonadotropin-releasing hormone therapy is associated with earlier spermatogenesis compared to combined gonadotropin therapy in patients with congenital hypogonadotropic hypogonadism
Abstract
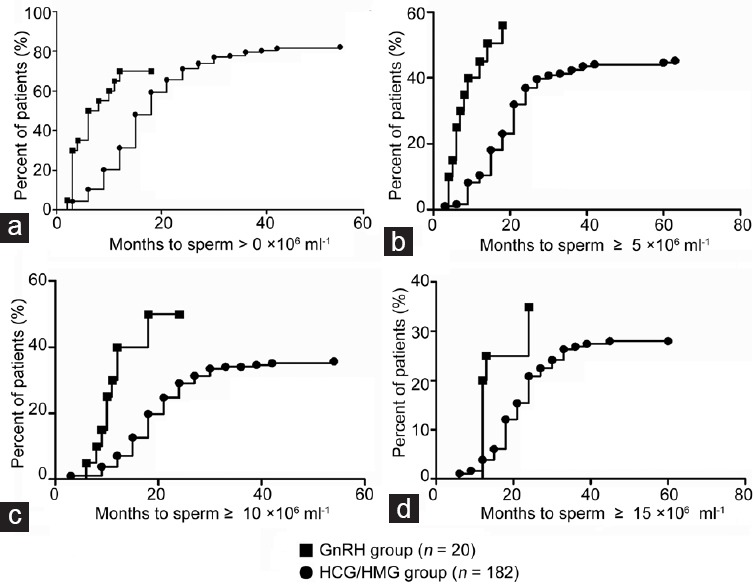
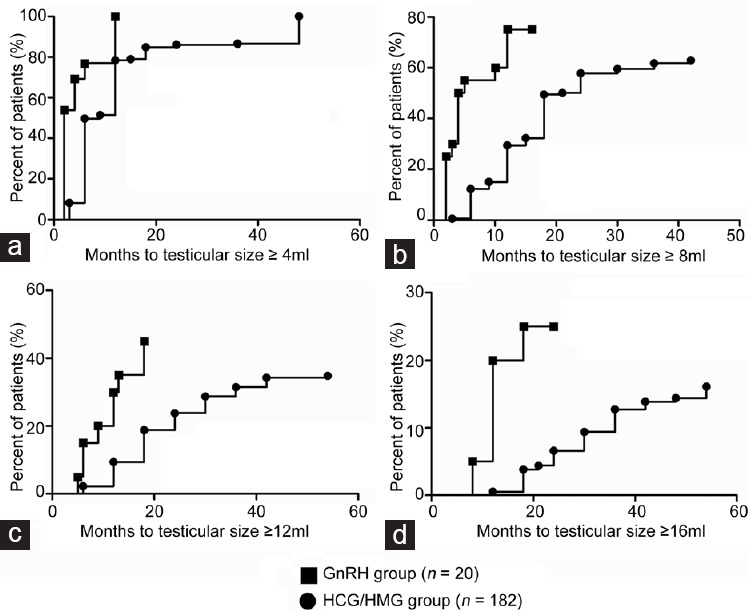
Both pulsatile gonadotropin-releasing hormone (GnRH) infusion and combined gonadotropin therapy (human chorionic gonadotropin and human menopausal gonadotropin [HCG/HMG]) are effective to induce spermatogenesis in male patients with congenital hypogonadotropic hypogonadism (CHH). However, evidence is lacking as to which treatment strategy is better. This retrospective cohort study included 202 patients with CHH: twenty had received pulsatile GnRH and 182 had received HCG/HMG. Patients had received therapy for at least 12 months. The total follow-up time was 15.6 ± 5.0 months (range: 12-27 months) for the GnRH group and 28.7 ± 13.0 months (range: 12-66 months) for the HCG/HMG group. The median time to first sperm appearance was 6 months (95% confidence interval [CI]: 1.6-10.4) in the GnRH group versus 18 months (95% CI: 16.4-20.0) in the HCG/HMG group (P < 0.001). The median time to achieve sperm concentrations ≥5 × 10 6 ml-1 was 14 months (95% CI: 5.8-22.2) in the GnRH group versus 27 months (95% CI: 18.9-35.1) in the HCG/HMG group (P < 0.001), and the median time to concentrations ≥10 × 10 6 ml-1 was 18 months (95% CI: 10.0-26.0) in the GnRH group versus 39 months (95% CI unknown) in the HCG/HMG group. Compared to the GnRH group, the HCG/HMG group required longer treatment periods to achieve testicular sizes of ≥4 ml, ≥8 ml, ≥12 ml, and ≥16 ml. Sperm motility (a + b + c percentage) evaluated in semen samples with concentrations >1 × 10 6 ml-1 was 43.7% ± 20.4% (16 samples) in the GnRH group versus 43.2% ± 18.1% (153 samples) in the HCG/HMG group (P = 0.921). Notably, during follow-up, the GnRH group had lower serum testosterone levels than the HCG/HMG group (8.3 ± 4.6 vs 16.2 ± 8.2 nmol l-1 , P < 0.001). Our study found that pulsatile GnRH therapy was associated with earlier spermatogenesis and larger testicular size compared to combined gonadotropin therapy. Additional prospective randomized studies would be required to confirm these findings.
Figures
References
-
- Rastrelli G, Corona G, Mannucci E, Maggi M. Factors affecting spermatogenesis upon gonadotropin-replacement therapy: a meta-analytic study. Andrology. 2014;2:794–808. - PubMed
-
- Buchter D, Behre HM, Kliesch S, Nieschlag E. Pulsatile GnRH or human chorionic gonadotropin/human menopausal gonadotropin as effective treatment for men with hypogonadotropic hypogonadism: a review of 42 cases. Eur J Endocrinol. 1998;139:298–303. - PubMed
-
- Liu L, Chaudhari N, Corle D, Sherins RJ. Comparison of pulsatile subcutaneous gonadotropin-releasing hormone and exogenous gonadotropins in the treatment of men with isolated hypogonadotropic hypogonadism. Fertil Steril. 1988;49:302–8. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
