

The burden of major adverse cardiac events in patients with coronary artery disease
- PMID: 28052754
- PMCID: PMC5210314
- DOI: 10.1186/s12872-016-0436-7
The burden of major adverse cardiac events in patients with coronary artery disease
Abstract
Background: Patients with a history of cardiovascular disease are at high risk of developing secondary major adverse cardiac events (MACE). This study aimed to identify independent predictors of MACE after hospital admission which could be used to identify of high-risk patients who may benefit from preventive strategies.
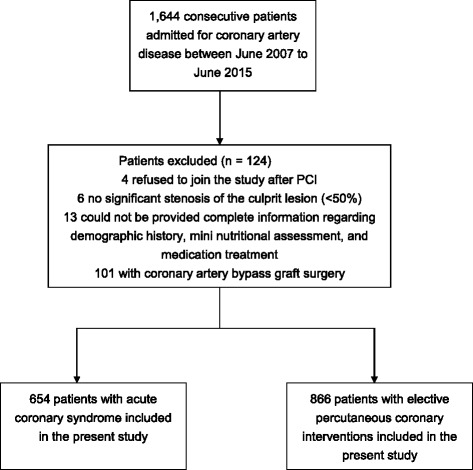
Methods: This study included 1,520 consecutive patients with coronary artery disease (CAD) (654 with acute coronary syndrome (ACS) and 866 with elective percutaneous coronary intervention (PCI) patients) who received PCI and/or stenting. MACE was defined as all-cause mortality or rehospitalization for a cardiovascular- related illness. Cardiovascular-related illnesses included heart failure, reinfarction (nonfatal), recurrence of angina pectoris and repeat PCI or coronary artery bypass graft.
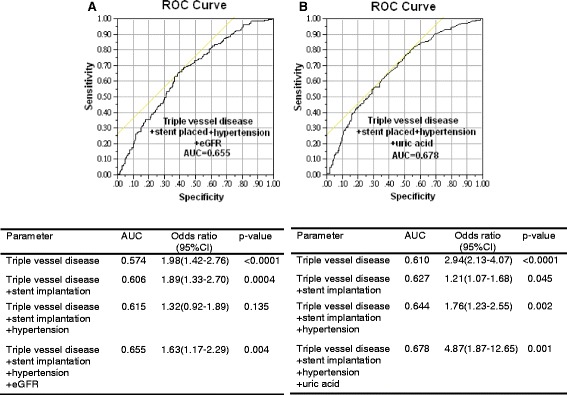
Results: During a mean follow-up period of 32 months, 558 of the 1,520 patients developed at least one MACE. Cox regression analysis showed that the baseline clinical and biochemical variables which associated with MACE were age, being illiterate, a widow or widower, and/or economically dependent, having triple vessel disease, stent implantation, anemia, and/or diabetes mellitus, waist to hip ratio (WHR), diastolic blood pressure, fasting glucose, total cholesterol, high-density lipoprotein cholesterol (HDL-C), creatinine, estimated glomerular filtration rate (eGFR), red blood cell count, hemoglobin, hematocrit, and mean corpuscular-hemoglobin concentration (MCHC) in ACS patients, and age, malnourished, and/or economically dependent, taking hypoglycemic medication, having triple vessel disease, stent implantation, anemia, diabetes mellitus, and/or hypertension, WHR, fasting glucose, HDL-C, uric acid, creatinine, eGFR, high-sensitivity C-reactive protein, mean corpuscular volume, and MCHC in elective PCI patients. Using multivariate Cox regression analysis, we found the MACE's independent factors are triple vessel disease, stent implantation, hypertension, and eGFR in ACS patients, and having triple vessel disease, stent implantation, hypertension, and uric acid in elective PCI patients.
Conclusions: Having triple vessel disease, stent implantation, hypertension, and eGFR or uric acid independently predicted MACE in patients with CAD after long-term follow-up. Fortunately, these factors are modifiable and should be identified and monitored early.
Keywords: Coronary artery disease; Major adverse cardiovascular events; Predictive factors.
Figures
References
-
- Directorate-general of budget, accounting and statistics Executive Yuan, Republic of China Statistical Yearbook of the Republic of China. Health. 2010;114:109–116.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
