

Cancer incidence and mortality risks in a large US Barrett's oesophagus cohort
- PMID: 28053055
- PMCID: PMC5827961
- DOI: 10.1136/gutjnl-2016-312223
Cancer incidence and mortality risks in a large US Barrett's oesophagus cohort
Abstract
Objective: Barrett's oesophagus (BE) increases the risk of oesophageal adenocarcinoma by 10-55 times that of the general population, but no community-based cancer-specific incidence and cause-specific mortality risk estimates exist for large cohorts in the USA.
Design: Within Kaiser Permanente Northern California (KPNC), we identified patients with BE diagnosed during 1995-2012. KPNC cancer registry and mortality files were used to estimate standardised incidence ratios (SIR), standardised mortality ratios (SMR) and excess absolute risks.
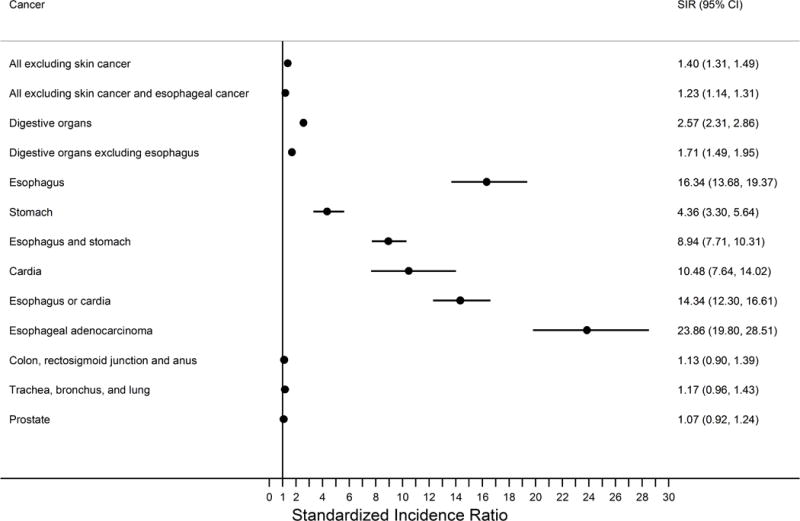
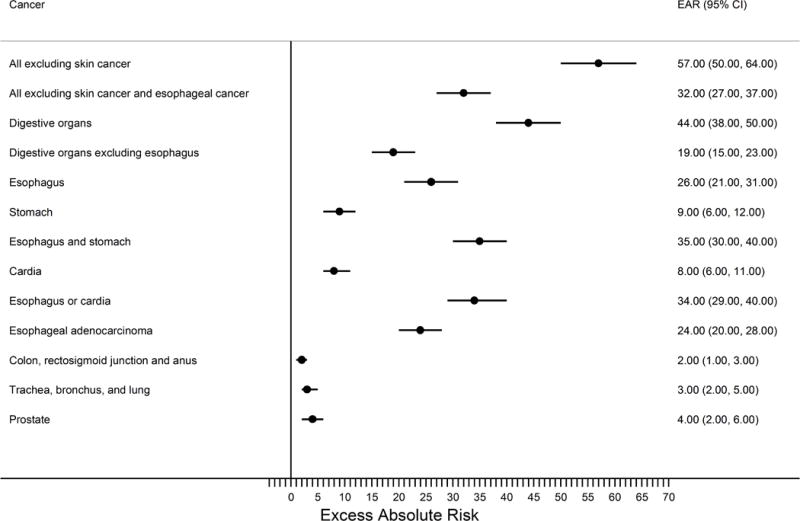
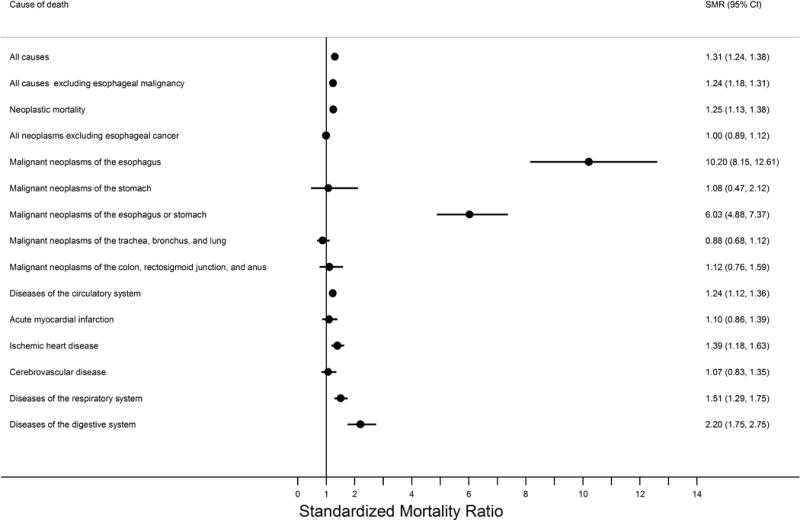
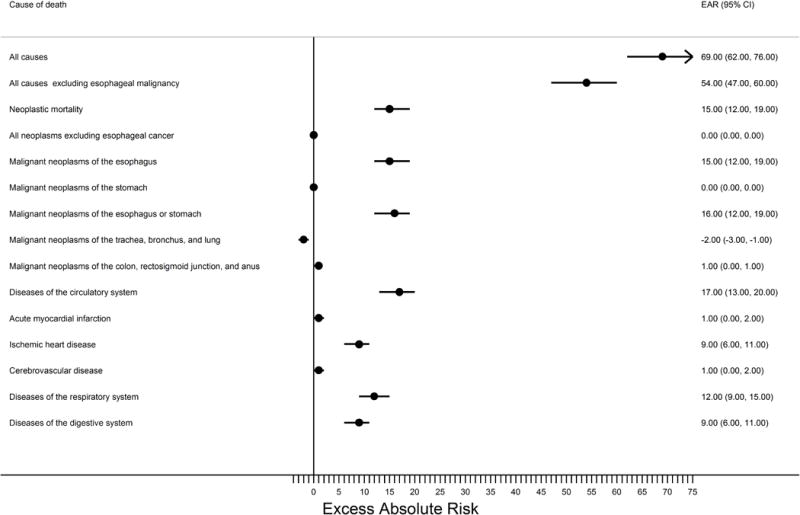
Results: There were 8929 patients with BE providing 50 147 person-years of follow-up. Compared with the greater KPNC population, patients with BE had increased risks of any cancer (SIR=1.40, 95% CI 1.31 to 1.49), which slightly decreased after excluding oesophageal cancer. Oesophageal adenocarcinoma risk was increased 24 times, which translated into an excess absolute risk of 24 cases per 10 000 person-years. Although oesophageal adenocarcinoma risk decreased with time since BE diagnosis, oesophageal cancer mortality did not, indicating that the true risk is stable and persistent with time. Relative risks of cardia and stomach cancers were increased, but excess absolute risks were modest. Risks of colorectal, lung and prostate cancers were unaltered. All-cause mortality was slightly increased after excluding oesophageal cancer (SMR=1.24, 95% CI 1.18 to 1.31), but time-stratified analyses indicated that this was likely attributable to diagnostic bias. Cause-specific SMRs were elevated for ischaemic heart disease (SMR=1.39, 95% CI 1.18 to 1.63), respiratory system diseases (SMR=1.51, 95% CI 1.29 to 1.75) and digestive system diseases (SMR=2.20 95% CI 1.75 to 2.75).
Conclusions: Patients with BE had a persistent excess risk of oesophageal adenocarcinoma over time, although their absolute excess risks for this cancer, any cancer and overall mortality were modest.
Keywords: BARRETT'S METAPLASIA; CANCER EPIDEMIOLOGY.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Spechler SJ, Robbins AH, Rubins HB, et al. Adenocarcinoma and Barrett’s esophagus. An overrated risk? Gastroenterology. 1984;87:927–33. - PubMed
-
- Polepalle SC, McCallum RW. Barrett’s esophagus. Current assessment and future perspectives. Gastroenterol Clin North Am. 1990;19:733–44. - PubMed
-
- Rana PS, Johnston DA. Incidence of adenocarcinoma and mortality in patients with Barrett’s oesophagus diagnosed between 1976 and 1986: implications for endoscopic surveillance. Dis Esophagus. 2000;13:28–31. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical