

Comparison of risk scoring systems for patients presenting with upper gastrointestinal bleeding: international multicentre prospective study
- PMID: 28053181
- PMCID: PMC5217768
- DOI: 10.1136/bmj.i6432
Comparison of risk scoring systems for patients presenting with upper gastrointestinal bleeding: international multicentre prospective study
Abstract
Objective: To compare the predictive accuracy and clinical utility of five risk scoring systems in the assessment of patients with upper gastrointestinal bleeding.
Design: International multicentre prospective study.
Setting: Six large hospitals in Europe, North America, Asia, and Oceania.
Participants: 3012 consecutive patients presenting over 12 months with upper gastrointestinal bleeding.
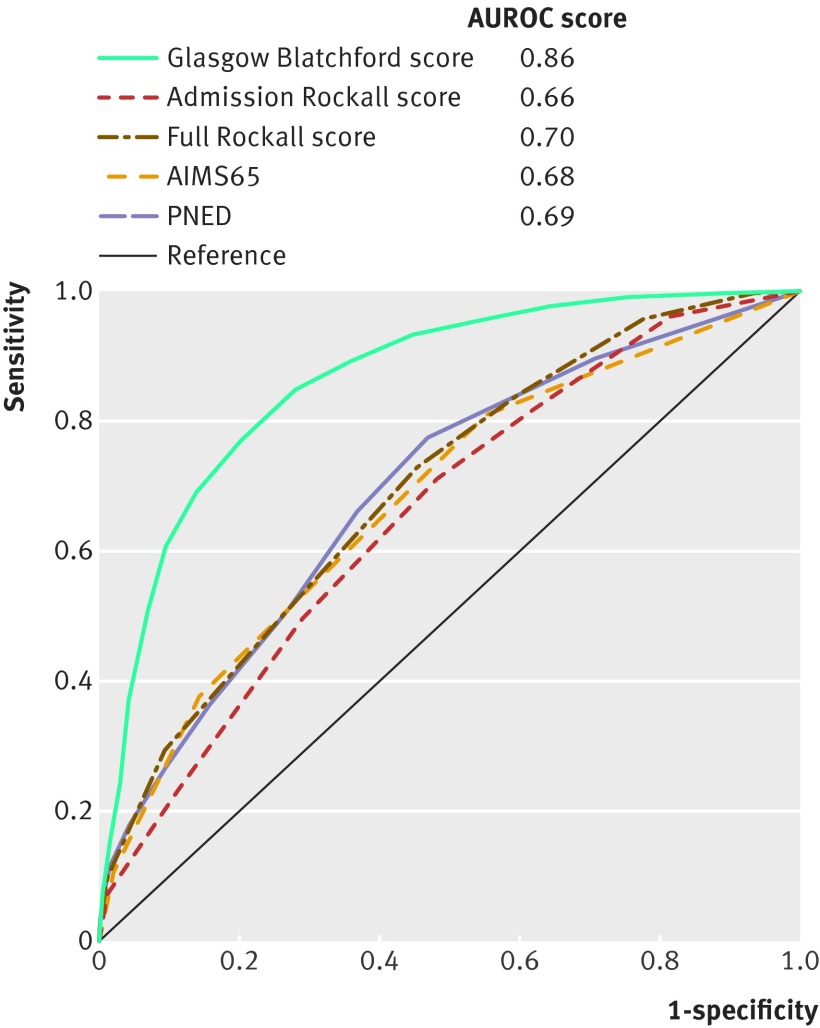
Main outcome measures: Comparison of pre-endoscopy scores (admission Rockall, AIMS65, and Glasgow Blatchford) and post-endoscopy scores (full Rockall and PNED) for their ability to predict predefined clinical endpoints: a composite endpoint (transfusion, endoscopic treatment, interventional radiology, surgery, or 30 day mortality), endoscopic treatment, 30 day mortality, rebleeding, and length of hospital stay. Optimum score thresholds to identify low risk and high risk patients were determined.
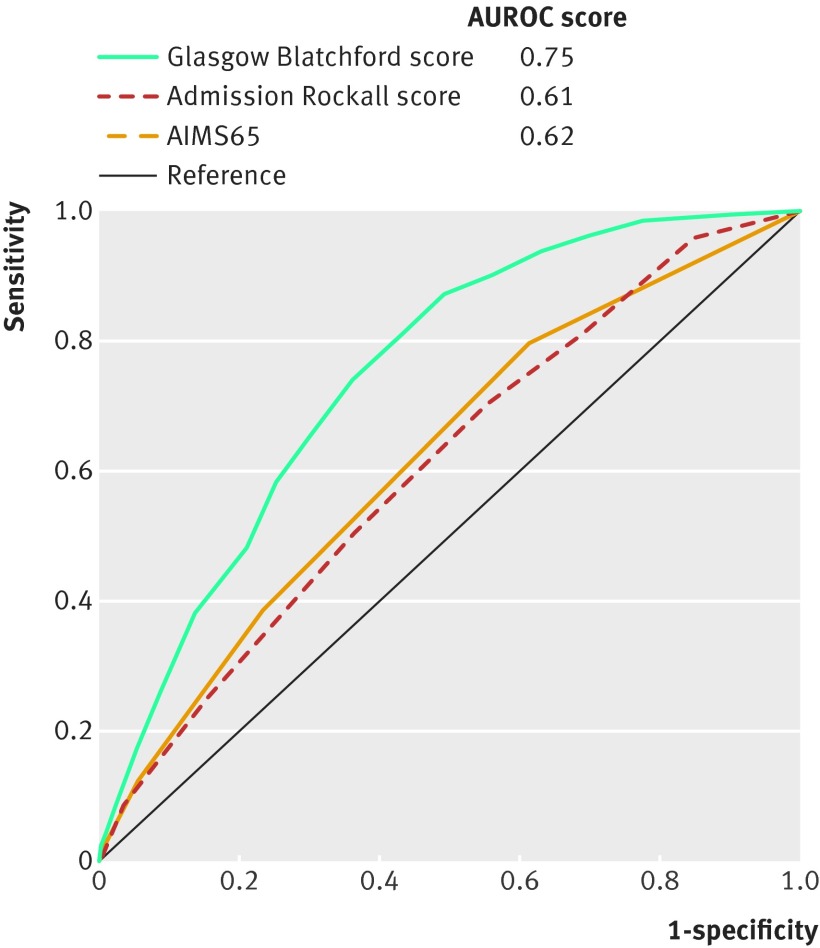
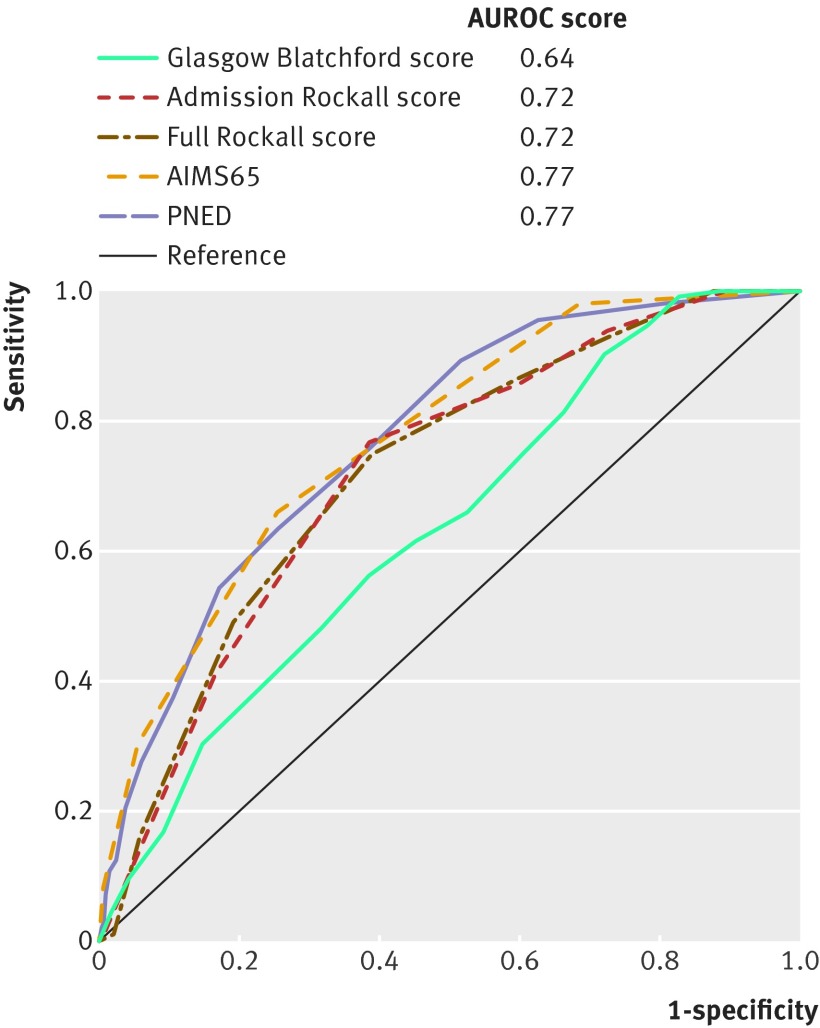
Results: The Glasgow Blatchford score was best (area under the receiver operating characteristic curve (AUROC) 0.86) at predicting intervention or death compared with the full Rockall score (0.70), PNED score (0.69), admission Rockall score (0.66, and AIMS65 score (0.68) (all P<0.001). A Glasgow Blatchford score of ≤1 was the optimum threshold to predict survival without intervention (sensitivity 98.6%, specificity 34.6%). The Glasgow Blatchford score was better at predicting endoscopic treatment (AUROC 0.75) than the AIMS65 (0.62) and admission Rockall scores (0.61) (both P<0.001). A Glasgow Blatchford score of ≥7 was the optimum threshold to predict endoscopic treatment (sensitivity 80%, specificity 57%). The PNED (AUROC 0.77) and AIMS65 scores (0.77) were best at predicting mortality, with both superior to admission Rockall score (0.72) and Glasgow Blatchford score (0.64; P<0.001). Score thresholds of ≥4 for PNED, ≥2 for AIMS65, ≥4 for admission Rockall, and ≥5 for full Rockall were optimal at predicting death, with sensitivities of 65.8-78.6% and specificities of 65.0-65.3%. No score was helpful at predicting rebleeding or length of stay.
Conclusions: The Glasgow Blatchford score has high accuracy at predicting need for hospital based intervention or death. Scores of ≤1 appear the optimum threshold for directing patients to outpatient management. AUROCs of scores for the other endpoints are less than 0.80, therefore their clinical utility for these outcomes seems to be limited.Trial registration Current Controlled Trials ISRCTN16235737.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare that: (1) no authors have support from any company for the submitted work; (2) no authors have relationships with any company that might have an interest in the submitted work (3) no author, their spouses, partners, or children have financial relationships that may be relevant to the submitted work and (4) no authors have any non-financial interests that may be relevant to the submitted work.
Figures
Comment in
-
Glasgow Blatchford score predicted intervention or death better than 4 other prediction models in upper GI bleeding.Ann Intern Med. 2017 Apr 18;166(8):JC47. doi: 10.7326/ACPJC-2017-166-8-047. Ann Intern Med. 2017. PMID: 28418549 No abstract available.
-
Authors' reply to Dib.BMJ. 2017 Jun 22;357:j3023. doi: 10.1136/bmj.j3023. BMJ. 2017. PMID: 28642273 No abstract available.
-
Utility of AIMS65 score in predicting mortality in patients presenting with upper gastrointestinal bleeding.BMJ. 2017 Jun 22;357:j3019. doi: 10.1136/bmj.j3019. BMJ. 2017. PMID: 28642350 No abstract available.
References
-
- Rockall TA, Logan RFA, Devlin HB, Northfield TC. Incidence of and mortality from acute upper gastrointestinal haemorrhage in the UK. BMJ 1995;311:222-6. 10.1136/bmj.311.6999.222 pmid:7627034. - DOI - PMC - PubMed
-
- Blatchford O, Davidson LA, Murray WR, Blatchford M, Pell J. Acute upper gastrointestinal haemorrhage in west of Scotland: case ascertainment study. BMJ 1997;315:510-4. 10.1136/bmj.315.7107.510 pmid:9329304. - DOI - PMC - PubMed
-
- Hearnshaw SA, Logan RFA, Lowe D, Travis SP, Murphy MF, Palmer KR. Acute upper gastrointestinal bleeding in the UK: patient characteristics, diagnoses and outcomes in the 2007 UK audit. Gut 2011;60:1327-35. 10.1136/gut.2010.228437 pmid:21490373. - DOI - PubMed
-
- Rockall TA, Logan RFA, Devlin HB, Northfield TC. Risk assessment after acute upper gastrointestinal haemorrhage. Gut 1996;38:316-21. 10.1136/gut.38.3.316 pmid:8675081. - DOI - PMC - PubMed
-
- Marmo R, Koch M, Cipolletta L, et al. Italian registry on upper gastrointestinal bleeding (Progetto Nazionale Emorragie Digestive--PNED 2). Predicting mortality in non-variceal upper gastrointestinal bleeders: validation of the Italian PNED Score and Prospective Comparison with the Rockall Score. Am J Gastroenterol 2010;105:1284-91. 10.1038/ajg.2009.687 pmid:20051943. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical