

Evaluation of left pulmonary artery sling, associated cardiovascular anomalies, and surgical outcomes using cardiovascular computed tomography angiography
- PMID: 28053308
- PMCID: PMC5215389
- DOI: 10.1038/srep40042
Evaluation of left pulmonary artery sling, associated cardiovascular anomalies, and surgical outcomes using cardiovascular computed tomography angiography
Abstract
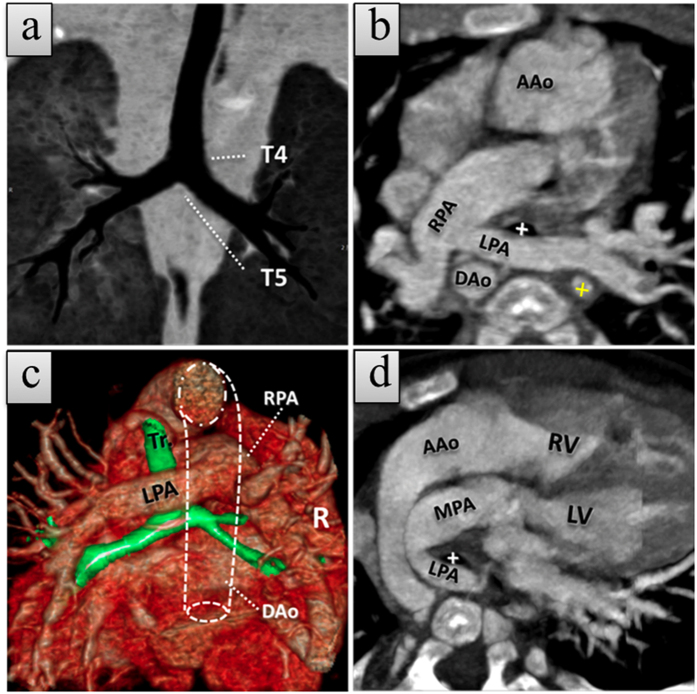
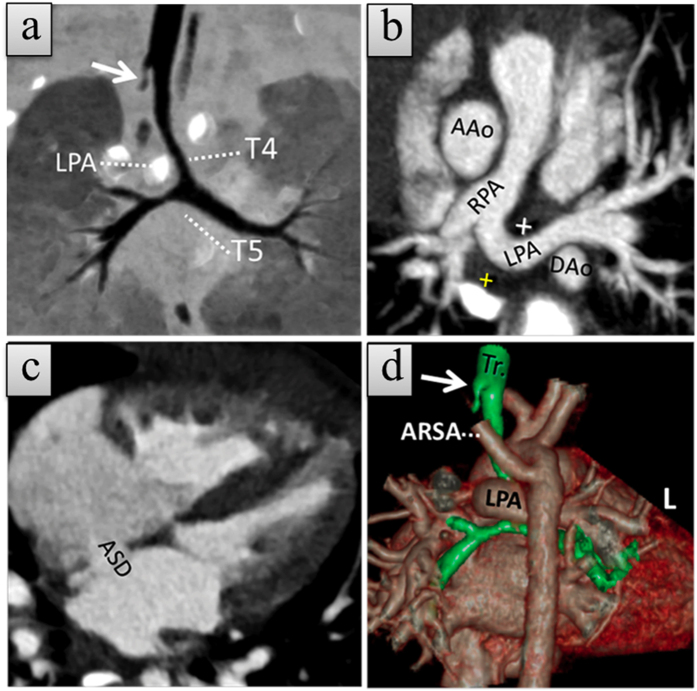
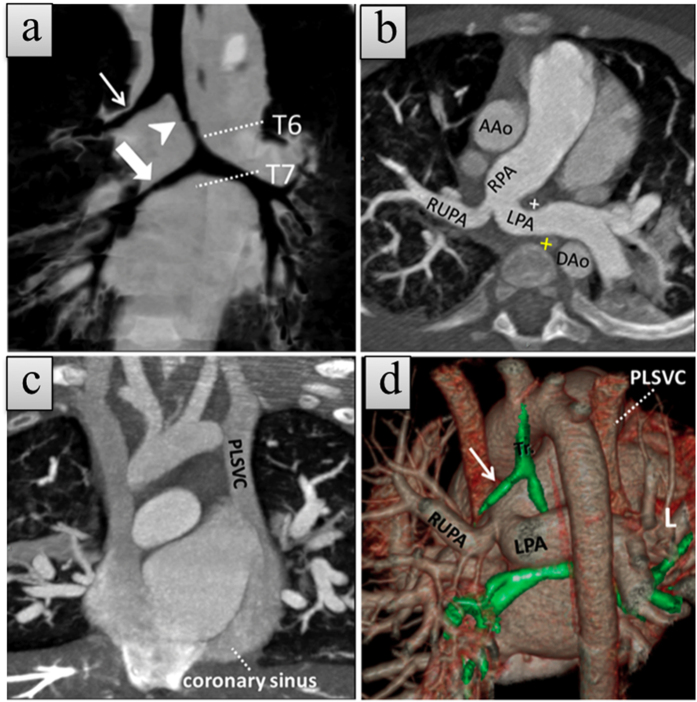
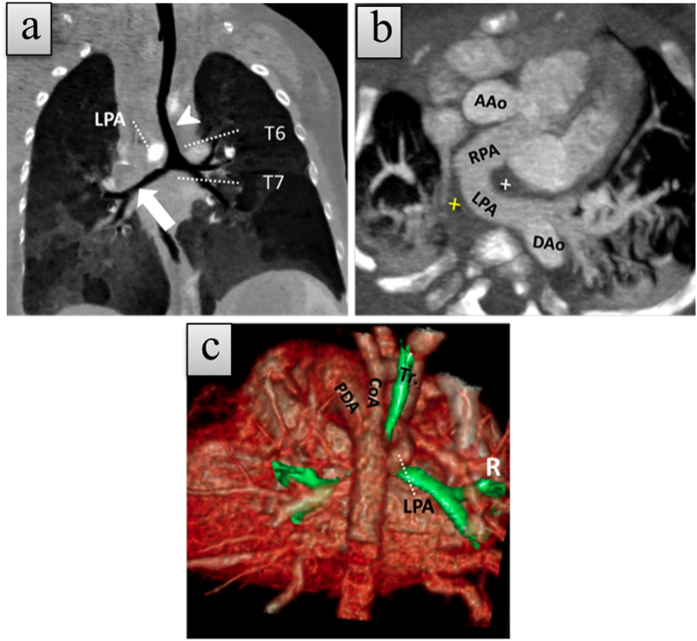
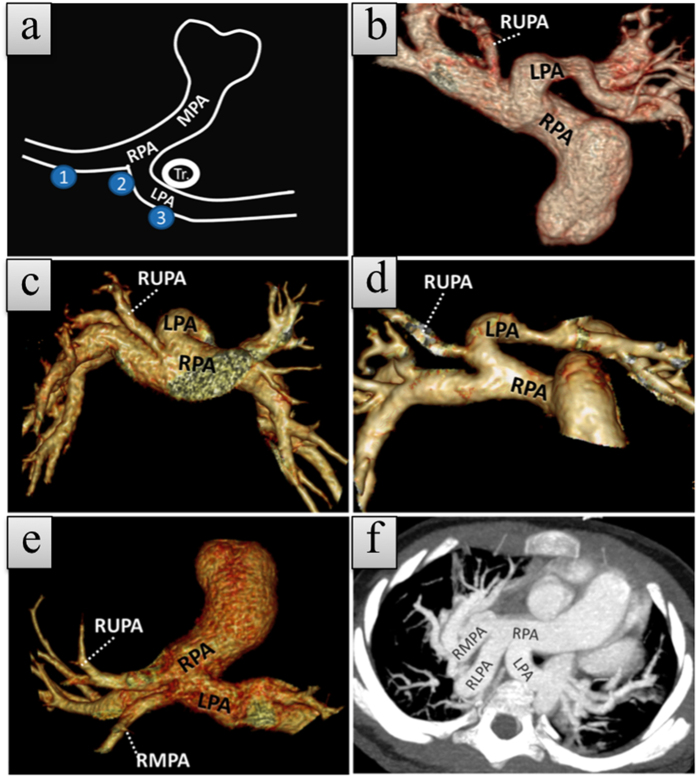
We evaluated the prevalence, image appearance, associated cardiovascular anomalies, and surgical outcomes of left pulmonary artery sling (LPAS) using cardiovascular computed tomography angiography (CCTA). A retrospective search of patients from our database between October 2007 and December 2014 identified 52,200 patients with congenital heart diseases (CHD) referred for CCTA, echocardiography, or magnetic resonance imaging. Clinical information, CCTA findings, associated cardiovascular anomalies, and surgical outcomes were analyzed. We showed a hospital-based prevalence of 71 patients with LPAS (0.14%, 71/52,200) among CHD patients. Of these, 47 patients with CCTA examinations were assessed further. Most patients (40/47, 85%) had associated cardiovascular anomalies, of which ventricular septal defects (22/47, 47%), atrial septal defects (20/47, 43%), patent ductus arteriosus (16/47, 34%), persistent left superior vena cava (14/47, 30%), and abnormal branching of the right pulmonary artery (ABRPA) (14/47, 30%) were most commonly identified. In total, 28 patients underwent LPA reanastomosis and/or tracheoplasty in our center, and 5 died. LPAS had a hospital-based prevalence of 0.14% among CHD patients. ABRPA is not uncommon and must be recognized. CCTA is a feasible method for demonstrating LPAS and its associated cardiovascular anomalies for an optimal pre-operative assessment of LPAS.
Figures
References
-
- Pawade A., de Leval M. R., Elliott M. J. & Stark J. Pulmonary artery sling. Ann Thorac Surg 54, 967–970 (1992). - PubMed
-
- Wells T. R., Gwinn J. L., Landing B. H. & Stanley P. Reconsideration of the anatomy of sling left pulmonary artery: the association of one form with bridging bronchus and imperforate anus. Anatomic and diagnostic aspects. J Pediatr Surg 23, 892–898 (1988). - PubMed
-
- Hu X. H., Pa M. E., Shen Q. L. & Huang G. Y. Multi-detector computed tomography evaluation of tracheobronchial anomaly in pediatric patients with left pulmonary artery sling. Chin Med J(Engl) 126, 2790–2792 (2013). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
