

Chronic central serous chorioretinopathy: long-term follow-up and vision-related quality of life
- PMID: 28053499
- PMCID: PMC5189979
- DOI: 10.2147/OPTH.S115685
Chronic central serous chorioretinopathy: long-term follow-up and vision-related quality of life
Abstract
Purpose: To describe the clinical findings and long-term outcome of patients with chronic central serous chorioretinopathy (cCSC).
Materials and methods: This was a retrospective case series in 52 eyes of 36 patients with a follow-up period of at least 1 year. Extensive ophthalmic examination and a validated questionnaire concerning vision-related quality of life (National Eye Institute Visual Function Questionnaire [NEI-VFQ]-39) were analyzed.
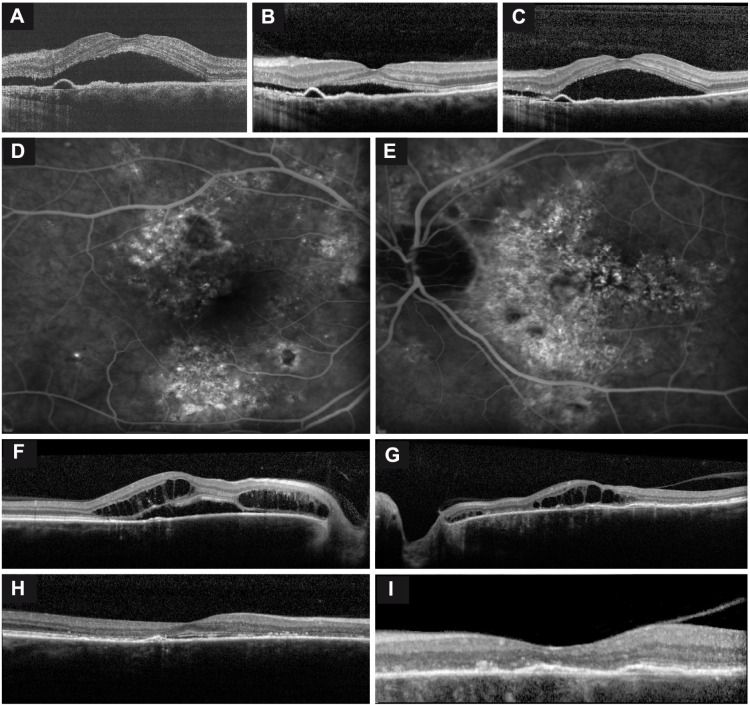
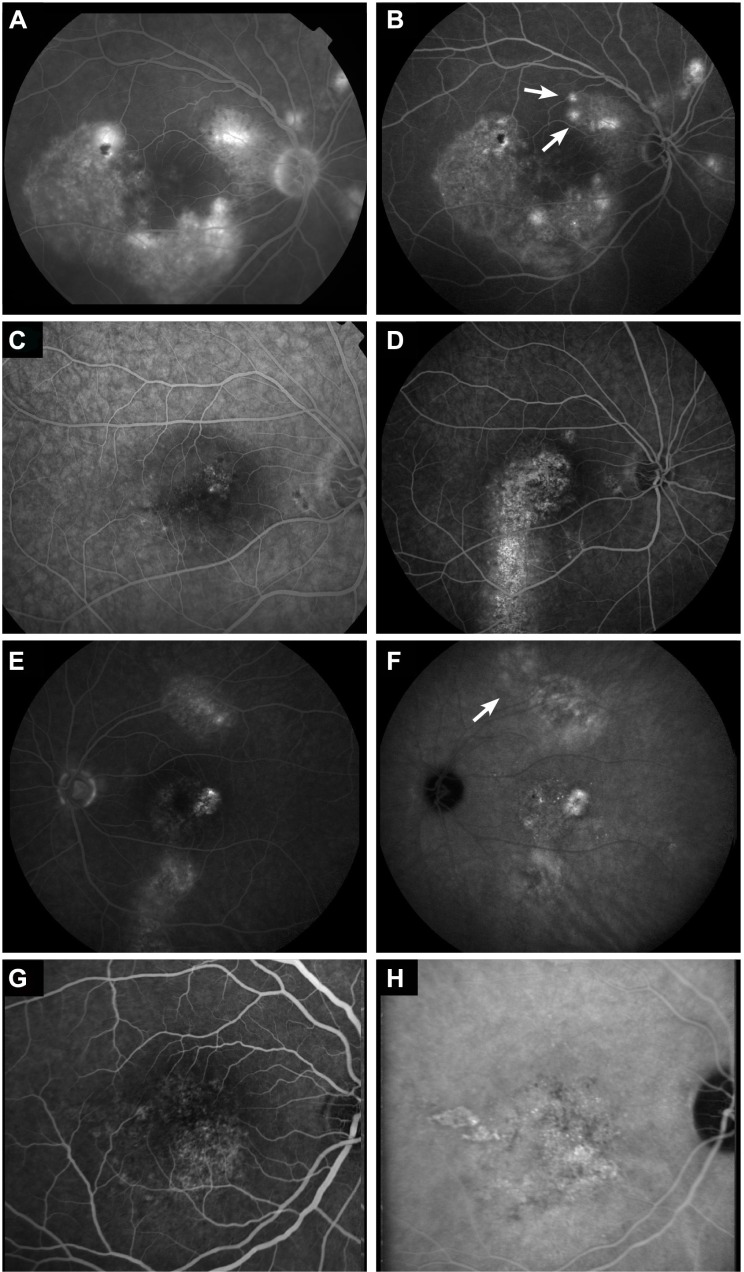
Results: Mean visual acuity showed a significant decline over time of 0.16 logarithm of minimum angle of resolution ([logMAR] range: -0.22 to 1.3; P=0.009) after a mean follow-up period of 10.6 years. Also, patients reported lower vision-related quality of life based on the NEI-VFQ-39 for almost all categories compared to healthy controls. Macular atrophy was diagnosed more often on optical coherence tomography compared to other diagnostic entities. Retinal pigment epithelium detachments in the macula were documented on optical coherence tomography in 56% of the patients. A significant thinning of foveal thickness was measured over time compared to unaffected fellow eyes (P=0.002). On long-term follow-up, 13 eyes (37%) showed an increase in number of hot spots on fluorescein angiography.
Conclusion: This study indicates that cCSC is a progressive disease in many patients, causing a progressive decline in visual acuity, accompanied by lower reported vision-related quality of life. In deciding whether or not to treat, the progressive nature of cCSC should be taken into account in this relatively young and often still professionally active patient group.
Keywords: NEI-VFQ-39; PDT; chronic central serous chorioretinopathy; micropulse laser; vision-related quality of life.
Conflict of interest statement
Dr Camiel JF Boon was supported by a Niels Stensen Fellowship. The authors report no conflicts of interest in this work.
Figures
References
-
- Liew G, Quin G, Gillies M, Fraser-Bell S. Central serous chorioretinopathy: a review of epidemiology and pathophysiology. Clin Exp Ophthalmol. 2013;41(2):201–214. - PubMed
-
- Guyer DR, Yannuzzi LA, Slakter JS, Sorenson JA, Ho A, Orlock D. Digital indocyanine green videoangiography of central serous chorioretinopathy. Arch Ophthalmol. 1994;112(8):1057–1062. - PubMed
-
- Prünte C, Flammer J. Choroidal capillary and venous congestion in central serous chorioretinopathy. Am J Ophthalmol. 1996;121(1):26–34. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
