

Cervical intramedullary immature teratoma with metastatic recurrence in an adult
- PMID: 28053710
- PMCID: PMC5129400
- DOI: 10.1038/scsandc.2015.6
Cervical intramedullary immature teratoma with metastatic recurrence in an adult
Erratum in
-
Erratum for Spinal Cord Series and Cases content published prior to July 2016.Spinal Cord Ser Cases. 2016 Jul 21;2:16019. doi: 10.1038/scsandc.2016.19. eCollection 2016. Spinal Cord Ser Cases. 2016. PMID: 31265710 Free PMC article.
Abstract
Study design: Case report.
Objectives: We present for the first time an adult patient with cervical intramedullary immature teratoma with metastatic recurrence.
Setting: Peking university Shenzhen Hospital, Shenzhen, China.
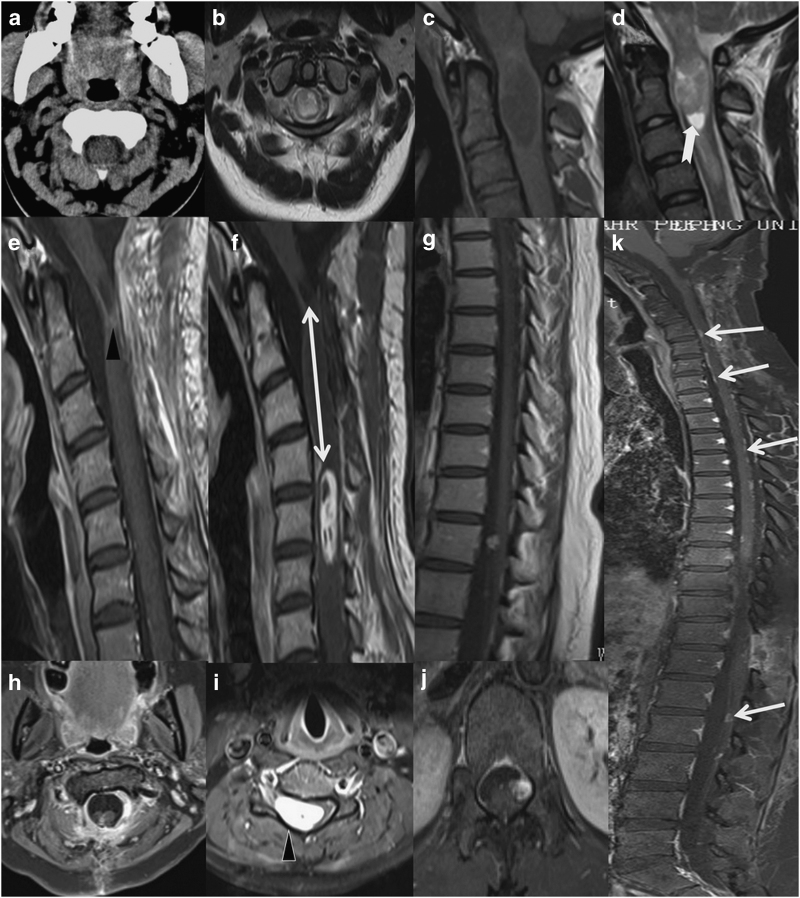
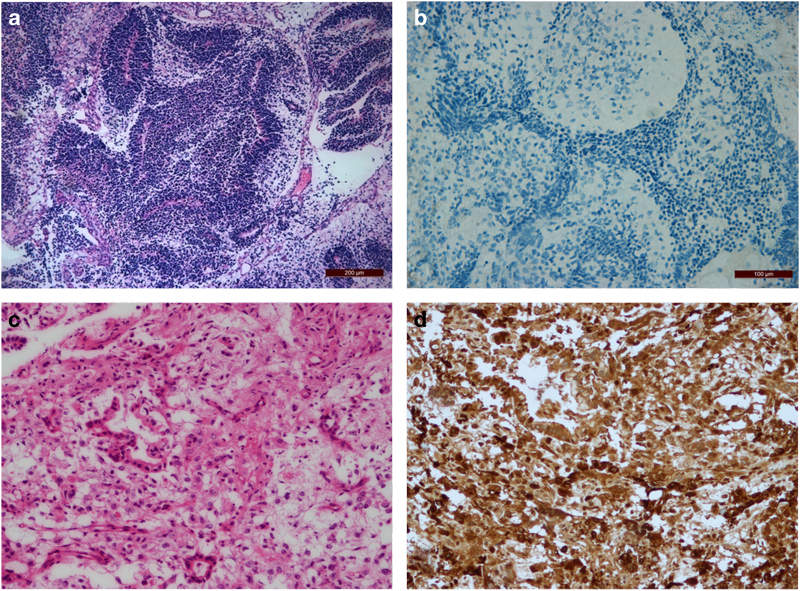
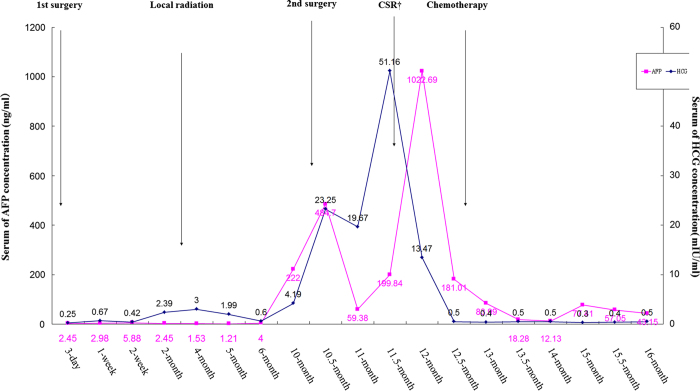
Methods: A 30-year-old woman presented with rapidly progressive quadriplegia. Magnetic resonance imaging (MRI) revealed an intramedullary tumor occupying C1-C2 of the upper spinal cord. An urgent operation, consisting of decompression by laminectomy and tumor gross resection, was performed under a preoperative diagnosis of spinal glioma. The histological diagnosis was immature teratoma. The patient received local radiotherapy after gross total resection. The serum alpha fetoprotein (AFP) and human chorionic gonadotropin (HCG) levels were normal postoperatively, until these were evaluated on the 10th month with neurological deterioration. Metastatic recurrences were demonstrated on MRI with lesions located at the levels of C5-C6 and T11-12. Removal of the second tumors was performed and the pathological examination identified a malignant germ cell tumor (yolk sac tumor). The patient was then referred to chemotherapy and radiotherapy.
Results: No tumor regrowth was encountered and the patient remained stable for 6 months after adjuvant therapy.
Conclusion: Immature teratoma should be included in the differential diagnosis of holocord tumors in the adult with rapidly progressing symptoms and if found should be radically excised if possible. Adjuvant therapy should be the salvage therapy for this recurrent tumor.
Figures
References
-
- Moon HJ , Shin BK , Kim JH , Kim JH , Kwon TH , Chung HS et al. Adult cervical intramedullary teratoma: first reported immature case. J Neurosurg Spine 2010; 13: 283–287. - PubMed
-
- Allsopp G , Sgouros S , Barber P , Walsh AR . Spinal teratoma: is there a place for adjuvant treatment? Two cases and a review of the literature. Br J Neurosurg 2000; 14: 482–488. - PubMed
-
- Ogawa K , Toita T , Nakamura K , Uno T , Onishi H , Itami J et al. Treatment and prognosis of patients with intracranial nongerminomatous malignant germ cell tumors: a multiinstitutional retrospective analysis of 41 patients. Cancer 2003; 98: 369–376. - PubMed
-
- Schild SE , Haddock MG , Scheithauer BW , Marks LB , Norman MG , Burger PC et al. Nongerminomatous germ cell tumors of the brain. Int J Radiat Oncol Biol Phys 1996; 36: 557–563. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
