

Diagnostic challenges in vacuolar myelopathy: a didactic case report
- PMID: 28053763
- PMCID: PMC5129393
- DOI: 10.1038/scsandc.2016.20
Diagnostic challenges in vacuolar myelopathy: a didactic case report
Abstract
Introduction: Because of the diagnostic complexity and potential pitfalls in interpreting test results, HIV-vacuolar myelopathy (HIVM) is far more often diagnosed postmortem than in vivo. In the era of highly active antiretroviral therapy (HAART), the topic of neuro-AIDS has become increasingly important. This case report covers some of the diagnostic problems encountered in vacuolar myelopathy based on magnetic resonance imaging (MRI) fiber-tracking pictures of the spine in a patient with HIVM, including a 1-year follow-up.
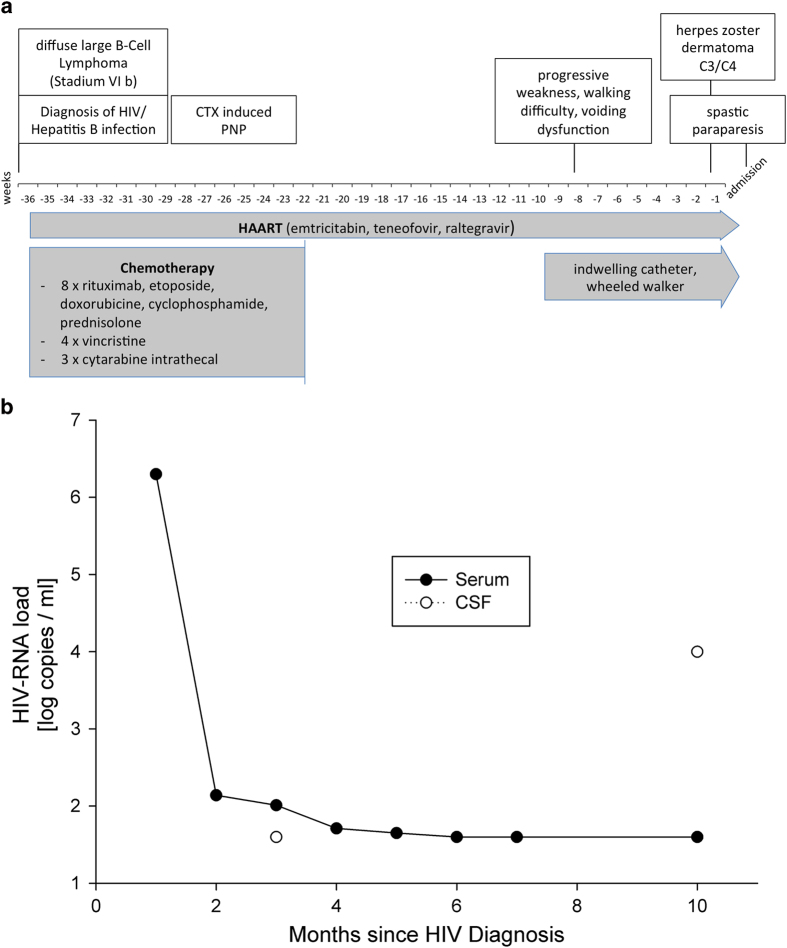
Case presentation: A 49-year-old man felt progressive weakness, and difficulties while walking, and he suffered from incomplete voiding. A week before admission, follicles appeared on the right side of his neck and shoulder. His medical history included a chronic HIV infection treated with HAART and a B-cell lymphoma in complete remission after chemotherapy. The initial exam revealed thoracic hyposensitivity level distal to dermatome Th9, spastic paraparesis of the lower limbs and herpes zoster infection in dermatome C3/C4. A lesion of the thoracic myelon could be ruled out in the MRI scan, chemotherapy-induced polyneuropathy was stable, and no acute opportunistic infection of the CNS was found. HIV load in cerebrospinal fluid (CSF) was markedly elevated. An HIV-associated vacuolar myelopathy was diagnosed, revealing the HIV itself as etiology.
Discussion: A negative or unspecific MRI scan excludes possible other causes, but by no means rules out HIV-related myelopathy. Furthermore, peripheral and central viral load should always be assessed to avoid missing a possible 'CSF HIV-escape'.
Keywords: Central nervous system infections; Disability; Infection; Neurological manifestations; Spinal cord.
Figures


References
-
- Dal Pan GJ, Glass JD, McArthur JC. Clinicopathologic correlations of HIV-1-associated vacuolar myelopathy: an autopsy-based case-control study. Neurology 1994; 44: 2159–2164. - PubMed
-
- Kwong Y-L, Yeung DYM, Chan JCW. Intrathecal chemotherapy for hematologic malignancies: drugs and toxicities. Ann Hematol 2008; 88: 193–201. - PubMed
-
- Cho TA, Vaitkevicius H. Infectious myelopathies. Continuum (Minneapolis Minn.) 2012; 18: 1351–1373. - PubMed
-
- Bizaare M, Dawood H, Moodley A. Vacuolar myelopathy: a case report of functional, clinical, and radiological improvement after highly active antiretroviral therapy. Int J Infect Dis 2008; 12: 442–444. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
