

Retro-odontoid mass without atlantoaxial instability causing cervical myelopathy: a case report of transdural surgical resection
- PMID: 28053768
- PMCID: PMC5129386
- DOI: 10.1038/scsandc.2016.25
Retro-odontoid mass without atlantoaxial instability causing cervical myelopathy: a case report of transdural surgical resection
Abstract
Introduction: Retro-odontoid mass rarely occur in patients with noninflammatory retro-odontoid lesions without atlantoaxial instability. We describe a rare case of retro-odontoid mass without atlantoaxial instability operated on by a transdural approach.
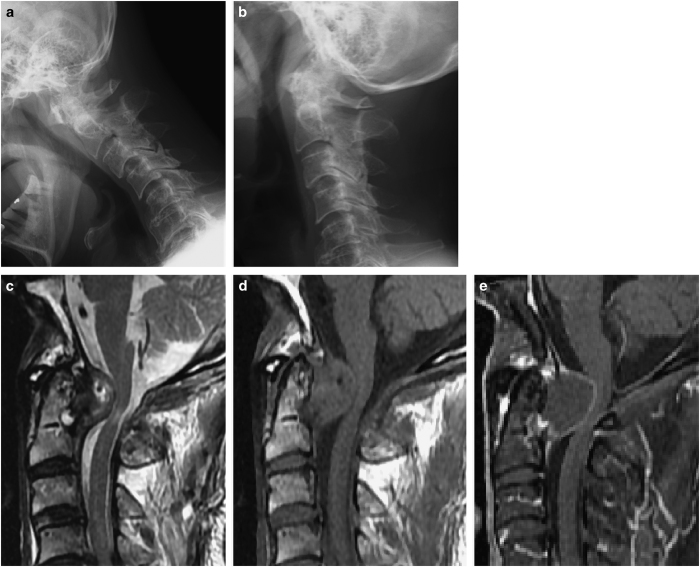
Case presentation: The patient was an 83-year-old man who presented with a retro-odontoid mass causing symptomatic cervical myelopathy. Preoperative magnetic resonance imaging (MRI) revealed that the mass was severely compressing the spinal cord. We operated on it via a C1 laminectomy and performed tumor resection by a transdural approach. Pathological findings from the operative specimen confirmed the diagnosis; histopathological examination revealed that the mass contained fibrinoid material, and collagenous tissue with myxoid changes, but no granulation or a granulomatous lesion. Postoperative MRI confirmed spinal cord decompression. The patient's symptoms were alleviated, and he has not had a recurrence or cervical instability in the 7 years since his surgery.
Discussion: We successfully used a transdural approach in the present case and have observed no recurrence for 7 years postoperatively. C1 laminectomy is reportedly beneficial, especially for elderly patients, given the risk of other surgical options using an anterior transoral approach or posterior fusion. However, most tumors do not attenuate after C1 laminectomy alone; hence, we think that tumor resection by the transdural approach is one effective method to perform enucleation of the tumor after C1 laminectomy.
Keywords: Bone; Spinal cord diseases.
Figures


References
-
- Cai CY, Palmer CA, Paramore CG. Exuberant transverse ligament degeneration causing high cervical myelopathy. J Spinal Disord 2001; 14: 84–88. - PubMed
-
- Chen TY, Lui TN. Retrodental fibrocartilaginous mass. Report of a case. Spine 1997; 22: 920–923. - PubMed
-
- Miller JD, al-Mefty O, Middleton TH 3rd. Synovial cyst at the craniovertebral junction. Surg Neurol 1989; 31: 239–242. - PubMed
-
- Sze G, Brant-Zawadzki MN, Wilson CR, Norman D, Newton TH. Pseudotumor of the craniovertebral junction associated with chronic subluxation: MR imaging studies. Radiology 1986; 161: 391–394. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
