

Complications, Not Minimally Invasive Surgical Technique, Are Associated with Increased Cost after Esophagectomy
- PMID: 28053785
- PMCID: PMC5178372
- DOI: 10.1155/2016/7690632
Complications, Not Minimally Invasive Surgical Technique, Are Associated with Increased Cost after Esophagectomy
Abstract
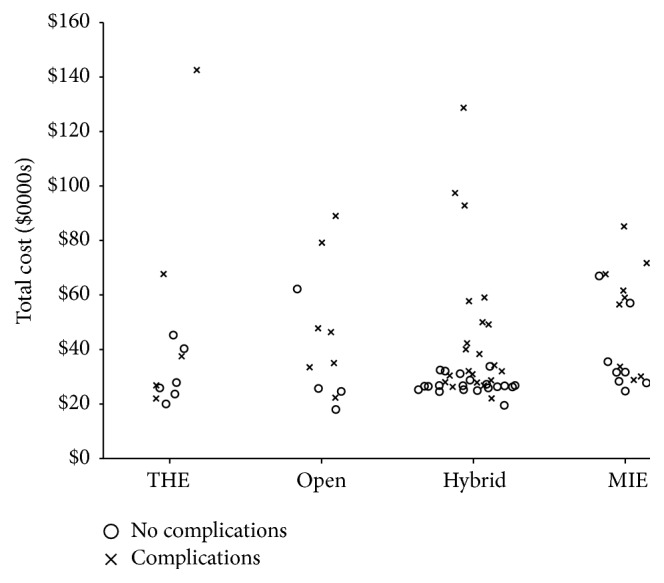
Background. Minimally invasive esophagectomy (MIE) techniques offer similar oncological and surgical outcomes to open methods. The effects of MIE on hospital costs are not well documented. Methods. We reviewed the electronic records of patients who underwent esophagectomy at a single academic institution between January 2012 and December 2014. Esophagectomy techniques were grouped into open, hybrid, MIE, and transhiatal (THE) esophagectomy. Univariate and multivariate analyses were performed to assess the impact of surgery on total hospital cost after esophagectomy. Results. 80 patients were identified: 11 THE, 11 open, 41 hybrid, and 17 MIE. Median total cost of the hospitalization was $31,375 and was similar between surgical technique groups. MIE was associated with higher intraoperative costs, but not total hospital cost. Multivariable analysis revealed that the presence of a complication, increased age, American Society of Anesthesiologists class IV (ASA4), and preoperative coronary artery disease (CAD) were associated with significantly increased cost. Conclusions. Despite the association of MIE with higher operation costs, the total hospital cost was not different between surgical technique groups. Postoperative complications and severe preoperative comorbidities are significant drivers of hospital cost associated with esophagectomy. Surgeons should choose technique based on clinical factors, rather than cost implications.
Conflict of interest statement
The authors have no competing interests regarding the publication of this paper.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
