

The impact of age on complications, survival, and cause of death following colon cancer surgery
- PMID: 28056465
- PMCID: PMC5294480
- DOI: 10.1038/bjc.2016.421
The impact of age on complications, survival, and cause of death following colon cancer surgery
Abstract
Background: Given scarce data regarding the relationship among age, complications, and survival beyond the 30-day postoperative period for oncology patients in the United States, this study identified age-related differences in complications and the rate and cause of 1-year mortality following colon cancer surgery.
Methods: The NY State Cancer Registry and Statewide Planning and Research Cooperative System identified stage I-III colon cancer resections (2004-2011). Multivariable logistic regression and survival analyses assessed the relationship among age (<65, 65-74, ⩾75), complications, 1-year survival, and cause of death.
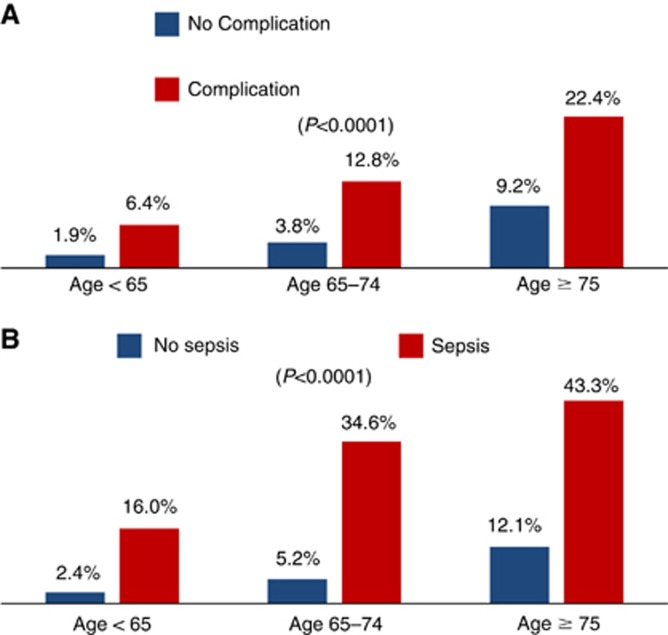
Results: Among 24 426 patients surviving >30 days, 1-year mortality was 8.5%. Older age groups had higher complication rates, and older age and complications were independently associated with 1-year mortality (P<0.0001). Increasing age was associated with a decrease in the proportion of deaths from colon cancer with a concomitant increase in the proportion of deaths from cardiovascular disease. Older age and sepsis were independently associated with higher risk of colon cancer-specific death (65-74: HR=1.59, 95% CI=1.26-2.00; ⩾75: HR=2.57, 95% CI=2.09-3.16; sepsis: HR=2.58, 95% CI=2.13-3.11) and cardiovascular disease-specific death (65-74: HR=3.72, 95% CI=2.29-6.05; ⩾75: HR=7.02, 95% CI=4.44-11.10; sepsis: HR=2.33, 95% CI=1.81-2.99).
Conclusions: Older age and sepsis are associated with higher 1-year overall, cancer-specific, and cardiovascular-specific mortality, highlighting the importance of geriatric assessment, multidisciplinary care, and cardiovascular optimisation for older patients and those with infectious complications.
Conflict of interest statement
FJF received personal fees from UpToDate unrelated to the current work. The other authors have no conflicts of interest to report. Oral presentation at 2016 American Society of Clinical Oncology Annual Meeting, Chicago, IL, 6 June 2016.
Figures
References
-
- Aquina CT, Blumberg N, Becerra AZ, Boscoe FP, Schymura MJ, Noyes K, Monson JR, Fleming FJ (2016. a) Association among blood transfusion, sepsis, and decreased long-term survival after colon cancer resection. Ann Surg; e-pub ahead of print 14 September 2016; doi:10.1097/SLA.0000000000001990. - PubMed
-
- Aquina CT, Blumberg N, Probst CP, Becerra AZ, Hensley BJ, Iannuzzi JC, Gonzalez MG, Deeb AP, Noyes K, Monson JR, Fleming FJ (2015. a) Significant variation in blood transfusion practice persists following upper GI cancer resection. J Gastrointest Surg 19(11): 1927–1937. - PubMed
-
- Aquina CT, Blumberg N, Probst CP, Becerra AZ, Hensley BJ, Noyes K, Monson JR, Fleming FJ (2016. b) Large variation in blood transfusion use after colorectal resection: a call to action. Dis Colon Rectum 59(5): 411–418. - PubMed
-
- Aquina CT, Kelly KN, Probst CP, Iannuzzi JC, Noyes K, Langstein HN, Monson JR, Fleming FJ (2015. b) Surgeon volume plays a significant role in outcomes and cost following open incisional hernia repair. J Gastrointest Surg 19(1): 100–110. - PubMed
-
- Aquina CT, Probst CP, Becerra AZ, Hensley BJ, Iannuzzi JC, Noyes K, Monson JR, Fleming FJ (2016. c) High variability in nosocomial clostridium difficile infection rates across hospitals after colorectal resection. Dis Colon Rectum 59(4): 323–331. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
