

Case report: whole exome sequencing of primary cardiac angiosarcoma highlights potential for targeted therapies
- PMID: 28056866
- PMCID: PMC5217318
- DOI: 10.1186/s12885-016-3000-z
Case report: whole exome sequencing of primary cardiac angiosarcoma highlights potential for targeted therapies
Abstract
Background: Primary cardiac angiosarcomas are rare, but they are the most aggressive type of primary cardiac neoplasms. When patients do present, it is with advanced pulmonary and/or cardiac symptoms. Therefore, many times the correct diagnosis is not made at the time of initial presentation. These patients have metastatic disease and the vast majority of these patients die within a few months after diagnosis. Currently the treatment choices are limited and there are no targeted therapies available.
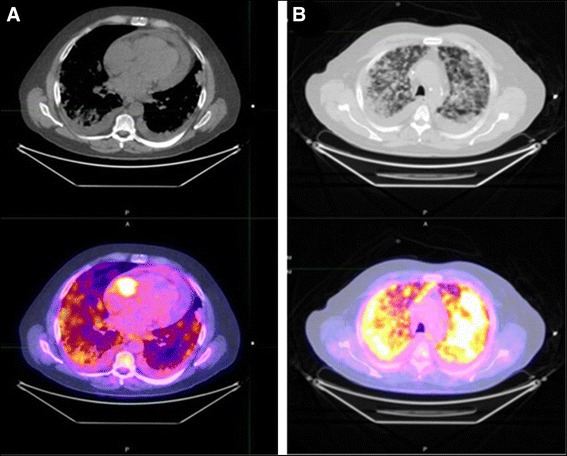
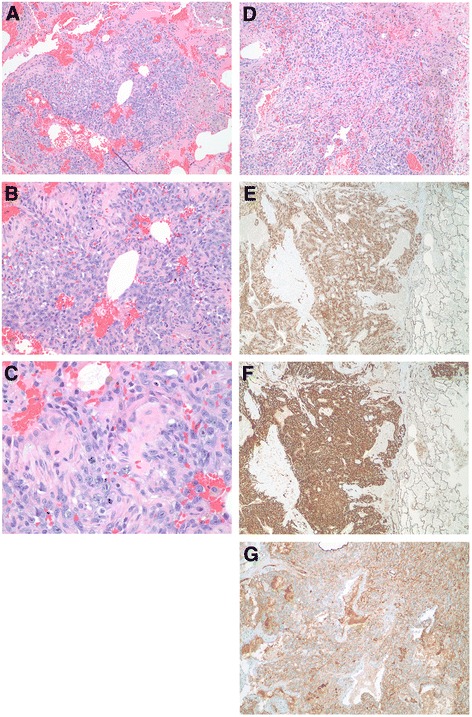
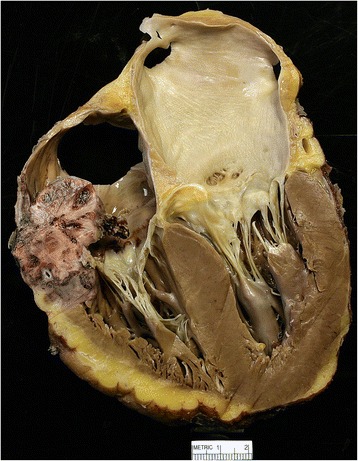
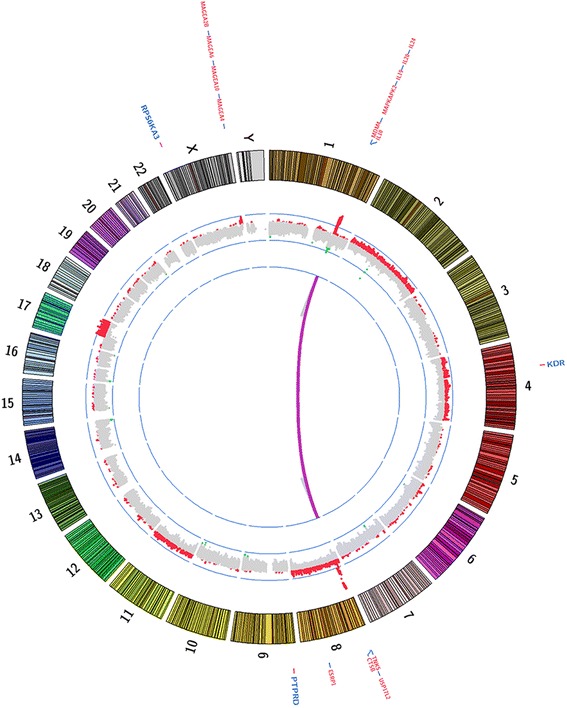
Case presentation: A 56-year-old male presented with shortness of breath, night sweats, and productive cough for a month. Workup revealed pericardial effusion and multiple bilateral pulmonary nodules suspicious for metastatic disease. Transthoracic echocardiogram showed a large pericardial effusion and a large mass in the base of the right atrium. Results of biopsy of bilateral lung nodules established a diagnosis of primary cardiac angiosarcoma. Aggressive pulmonary disease caused rapid deterioration; the patient went on hospice and subsequently died. Whole exome sequencing of the patient's postmortem tumor revealed a novel KDR (G681R) mutation, and focal high-level amplification at chromosome 1q encompassing MDM4, a negative regulator of TP53.
Conclusion: Mutations in KDR have been reported previously in angiosarcomas. Previous studies also demonstrated that KDR mutants with constitutive KDR activation could be inhibited with specific KDR inhibitors in vitro. Thus, patients harboring activating KDR mutations could be candidates for treatment with KDR-specific inhibitors.
Keywords: Activating gene mutation; Cardiac angiosarcoma; Targeted therapies; Whole exome sequencing.
Figures
References
-
- Lam KY, Dickens P, Chan AC. Tumors of the heart. A 20-year experience with a review of 12,485 consecutive autopsies. Arch Pathol Lab Med. 1993;117(10):1027–31. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
