

Solitary plasmacytoma: population-based analysis of survival trends and effect of various treatment modalities in the USA
- PMID: 28056880
- PMCID: PMC5216567
- DOI: 10.1186/s12885-016-3015-5
Solitary plasmacytoma: population-based analysis of survival trends and effect of various treatment modalities in the USA
Erratum in
-
Erratum to: Solitary plasmacytoma: population-based analysis of survival trends and effect of various treatment modalities in the USA.BMC Cancer. 2017 Jun 23;17(1):443. doi: 10.1186/s12885-017-3427-x. BMC Cancer. 2017. PMID: 28645258 Free PMC article. No abstract available.
Abstract
Background: Solitary plasmacytoma (SP) is a localized neoplastic plasma cell disorder with an annual incidence of less than 450 cases. Given the rarity of this disorder, it is difficult to conduct large-scale population studies. Consequently, very limited information on the disorder is available, making it difficult to estimate the incidence and survival rates. Furthermore, limited information is available on the efficacy of various treatment modalities in relation to primary tumor sites.
Methods: The data for this retrospective study were drawn from the Surveillance, Epidemiology and End Results (SEER) database, which comprises 18 registries; patient demographics, treatment modalities and survival rates were obtained for those diagnosed with SP from 1998 to 2007. Various prognostic factors were analyzed via Kaplan-Meier analysis and log-rank test, with 5-year relative survival rate defined as the primary outcome of interest. Cox regression analysis was employed in the multivariate analysis.
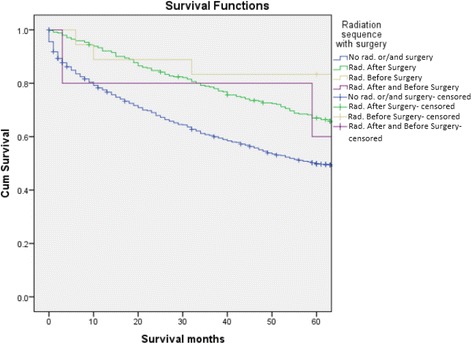
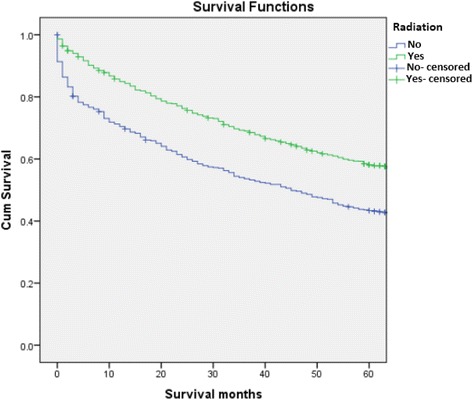
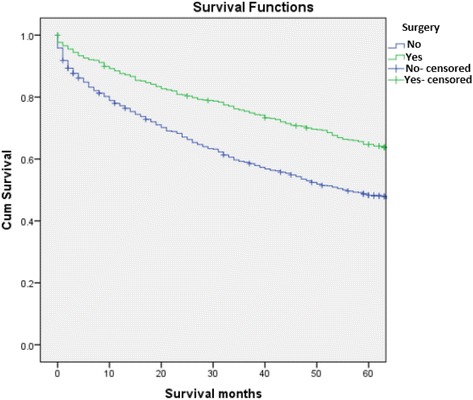
Results: The SEER search from 1998 to 2007 yielded records for 1691 SP patients. The median age at diagnosis was 63 years. The patient cohort was 62.4% male, 37.6% female, 80% Caucasian, 14.6% African American and 5.4% other races. Additionally, 57.8% had osseous plasmacytoma, and 31.9% had extraosseous involvement. Unspecified plasmacytoma was noted in 10.2% of patients. The most common treatment modalities were radiotherapy (RT) (48.8%), followed by combination surgery with RT (21.2%) and surgery alone (11.6%). Univariate analysis of prognostic factors revealed that the survival outcomes were better for younger male patients who received RT with surgery (p < 0.05). Additionally, patients who received neoadjuvant RT had increased survival rates compared to those receiving adjuvant RT (86% vs 73%, p < 0.05). Furthermore, the analyses revealed that 5-year survival rates for patients with axial plasmacytoma were superior when RT was combined with surgery (p < 0.05). In the multivariate analysis, age <60 years and treatment with either RT or surgery showed superior survival rates. Progression to multiple myeloma (MM) was noted in 551 patients. Age >60 years was associated with a lower 5-year survival in patients who progressed to MM compared to those who were diagnosed initially with MM (15.1 vs 16.6%). Finally, those who received RT and progressed to MM still had a higher chance of survival than those who were diagnosed with MM initially and treated with RT/surgery (21.8% vs 15.9%, p < 0.05).
Conclusions: A review of the pertinent literature indicates that we provided the most comprehensive population-based analysis of SP to date. Moreover, our study contributes to the establishment of the optimal SP treatment modality, as RT is the favored option in frontline settings. Consensus is currently lacking regarding the benefits of combined treatment including surgery. Thus, the findings reported here elucidate the role of primary treatment modalities while also demonstrating the quantifiable benefits of combining RT with surgery in relation to different primary tumor sites. While our results are promising, they should be confirmed through further large-scale randomized studies.
Figures
References
-
- Dimopoulos MA, Moulopoulos LA, Maniatis A, Alexanian R. “Solitary plasmacytoma of bone and asymptomatic multiple myeloma,”. Blood. 2000;96(6):2037. - PubMed
-
- Dimopoulos MA, Hamilos G. “Solitary bone plasmacytoma and extramedullary plasmacytoma,” CurrentTreatment Options in Oncology. 2002; p. 255-9 - PubMed
-
- Knowling MA, Harwood AR, Bergsagel DE. Comparison of extramedullary plasmacytomas with solitary and multiple plasma cell tumors of bone. J Clin Oncol. 1983;1(4):255–262. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
