

Advance Directives and End-of-Life Care among Nursing Home Residents Receiving Maintenance Dialysis
- PMID: 28057703
- PMCID: PMC5338713
- DOI: 10.2215/CJN.07510716
Advance Directives and End-of-Life Care among Nursing Home Residents Receiving Maintenance Dialysis
Abstract
Background and objectives: Little is known about the relation between the content of advance directives and downstream treatment decisions among patients receiving maintenance dialysis. In this study, we determined the prevalence of advance directives specifying treatment limitations and/or surrogate decision-makers in the last year of life and their association with end-of-life care among nursing home residents.
Design, setting, participants, & measurements: Using national data from 2006 to 2007, we compared the content of advance directives among 30,716 nursing home residents receiving dialysis to 30,825 nursing home residents with other serious illnesses during the year before death. Among patients receiving dialysis, we linked the content of advance directives to Medicare claims to ascertain site of death and treatment intensity in the last month of life.
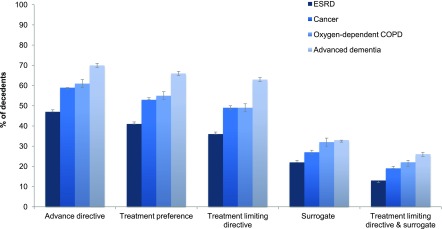
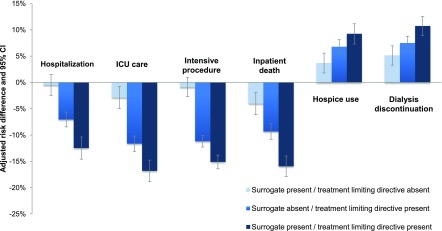
Results: In the last year of life, 36% of nursing home residents receiving dialysis had a treatment-limiting directive, 22% had a surrogate decision-maker, and 13% had both in adjusted analyses. These estimates were 13%-27%, 5%-11%, and 6%-13% lower, respectively, than for decedents with other serious illnesses. For patients receiving dialysis who had both a treatment-limiting directive and surrogate decision-maker, the adjusted frequency of hospitalization, intensive care unit admission, intensive procedures, and inpatient death were lower by 13%, 17%, 13%, and 14%, respectively, and hospice use and dialysis discontinuation were 5% and 7% higher compared with patients receiving dialysis lacking both components.
Conclusions: Among nursing home residents receiving dialysis, treatment-limiting directives and surrogates were associated with fewer intensive interventions and inpatient deaths, but were in place much less often than for nursing home residents with other serious illnesses.
Keywords: ESRD; Medicare; United States; advance directives; dialysis; hospice care; hospices; hospitalization; humans; inpatients; intensive care units; kidney failure, chronic; nursing homes; prevalence; renal dialysis; terminal care.
Copyright © 2017 by the American Society of Nephrology.
Figures
Comment in
-
Is the End in Sight for the "Don't Ask, Don't Tell" Approach to Advance Care Planning?Clin J Am Soc Nephrol. 2017 Mar 7;12(3):380-381. doi: 10.2215/CJN.00980117. Epub 2017 Feb 23. Clin J Am Soc Nephrol. 2017. PMID: 28232404 Free PMC article. No abstract available.
References
-
- Saran R, Li Y, Robinson B, Ayanian J, Balkrishnan R, Bragg-Gresham J, Chen JT, Cope E, Gipson D, He K, Herman W, Heung M, Hirth RA, Jacobsen SS, Kalantar-Zadeh K, Kovesdy CP, Leichtman AB, Lu Y, Molnar MZ, Morgenstern H, Nallamothu B, O’Hare AM, Pisoni R, Plattner B, Port FK, Rao P, Rhee CM, Schaubel DE, Selewski DT, Shahinian V, Sim JJ, Song P, Streja E, Kurella Tamura M, Tentori F, Eggers PW, Agodoa LY, Abbott KC: US Renal Data System 2014 Annual Data Report: Epidemiology of kidney disease in the United States. Am J Kidney Dis 66[Suppl 1]: S1–S305, 2015 - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
