

Prospective study of oral anticoagulants and risk of liver injury in patients with atrial fibrillation
- PMID: 28057799
- PMCID: PMC5429195
- DOI: 10.1136/heartjnl-2016-310586
Prospective study of oral anticoagulants and risk of liver injury in patients with atrial fibrillation
Abstract
Objective: To assess the risk of liver injury hospitalisation in patients with atrial fibrillation (AF) after initiation of direct oral anticoagulants (DOACs) or warfarin and to determine predictors of liver injury hospitalisation in this population.
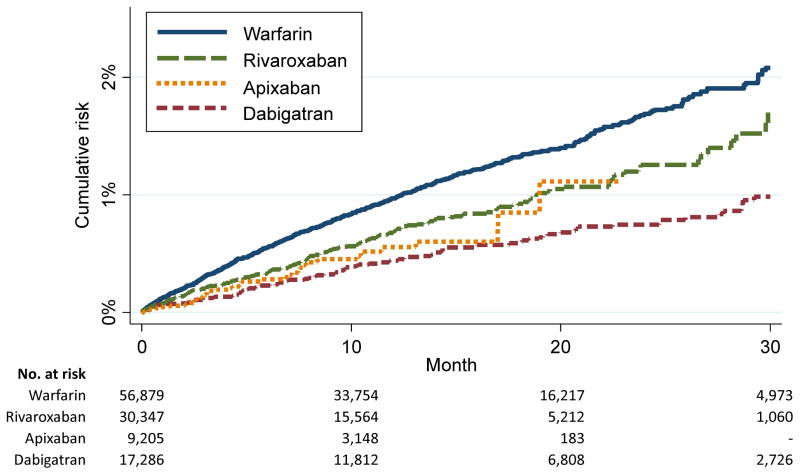
Methods: We studied 113 717 patients (mean age 70, 39% women) with AF included in the MarketScan Commercial and Medicare Supplemental databases with a first prescription for oral anticoagulation after 4 November 2011, followed through 31 December 2014. Of these, 56 879 initiated warfarin, 17 286 initiated dabigatran, 30 347 initiated rivaroxaban and 9205 initiated apixaban. Liver injury hospitalisation and comorbidities were identified from healthcare claims.
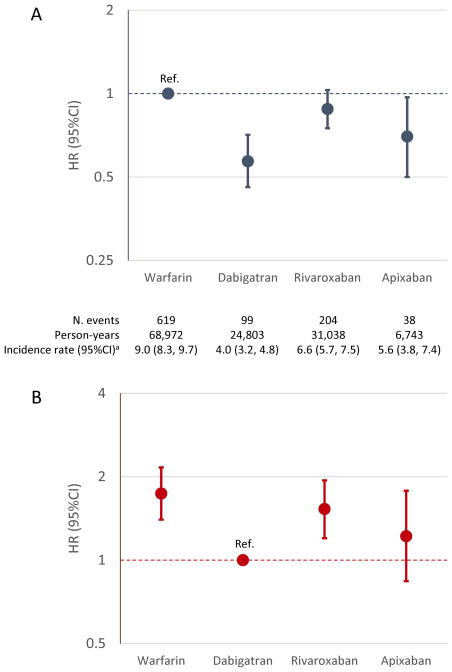
Results: During a median follow-up of 12 months, 960 hospitalisations with liver injury were identified. Rates of liver injury hospitalisation (per 1000 person-years) by oral anticoagulant were 9.0 (warfarin), 4.0 (dabigatran), 6.6 (rivaroxaban) and 5.6 (apixaban). After multivariable adjustment, liver injury hospitalisation rates were lower in initiators of DOACs compared with warfarin: HR (95% CI) of 0.57 (0.46 to 0.71), 0.88 (0.75 to 1.03) and 0.70 (0.50 to 0.97) for initiators of dabigatran, rivaroxaban, and apixaban, respectively (vs. warfarin). Compared with dabigatran initiators, rivaroxaban initiators had a 56% increased risk of liver injury hospitalisation (HR 1.56, 95% CI 1.22 to 1.99). In addition to type of anticoagulant, prior liver, gallbladder and kidney disease, cancer, anaemia, heart failure and alcoholism significantly predicted liver injury hospitalisation. A predictive model including these variables had adequate discriminative ability (C-statistic 0.67, 95% CI 0.64 to 0.70).
Conclusions: Among patients with non-valvular AF, DOACs were associated with lower risk of liver injury hospitalisation compared with warfarin, with dabigatran showing the lowest risk.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Competing interests: AA had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. LGSB is an employee of Optum.
Figures
Comment in
-
Drug-induced liver injury with oral anticoagulants: a threat or not?Heart. 2017 Jun;103(11):809-811. doi: 10.1136/heartjnl-2016-310983. Epub 2017 Feb 17. Heart. 2017. PMID: 28213369 No abstract available.
-
Liver injury with direct-acting anticoagulants: has the fog cleared?Heart. 2017 Dec;103(24):2010. doi: 10.1136/heartjnl-2017-311951. Heart. 2017. PMID: 29180521 No abstract available.
-
Oral anticoagulants and liver injury: the threat of uncontrolled confounding.Heart. 2018 Jan;104(1):84. doi: 10.1136/heartjnl-2017-311916. Heart. 2018. PMID: 29229784 Free PMC article. No abstract available.
References
-
- Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139–51. - PubMed
-
- Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883–91. - PubMed
-
- Granger CB, Alexander JH, McMurray JJV, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365:981–92. - PubMed
-
- Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369:2093–104. - PubMed
-
- Romanelli RJ, Nolting L, Dolginsky M, et al. Dabigatran versus warfarin for atrial fibrillation in real-world clinical practice: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2016;9:126–34. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical