

Dysphagia after vertical sleeve gastrectomy: Evaluation of risk factors and assessment of endoscopic intervention
- PMID: 28058017
- PMCID: PMC5175249
- DOI: 10.3748/wjg.v22.i47.10371
Dysphagia after vertical sleeve gastrectomy: Evaluation of risk factors and assessment of endoscopic intervention
Abstract
Aim: To evaluate the risks of medical conditions, evaluate gastric sleeve narrowing, and assess hydrostatic balloon dilatation to treat dysphagia after vertical sleeve gastrectomy (VSG).
Methods: VSG is being performed more frequently worldwide as a treatment for medically-complicated obesity, and dysphagia is common post-operatively. We hypothesize that post-operative dysphagia is related to underlying medical conditions or narrowing of the gastric sleeve. This is a retrospective, single institution study of consecutive patients who underwent sleeve gastrectomy from 2013 to 2015. Patients with previous bariatric procedures were excluded. Narrowing of a gastric sleeve includes: inability to pass a 9.6 mm gastroscope due to stenosis or sharp angulation or spiral hindering its passage.
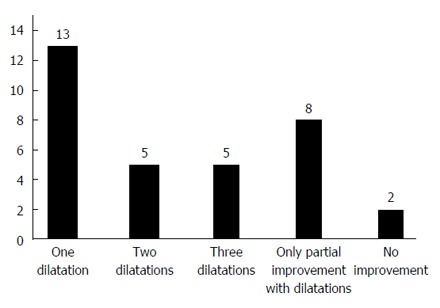
Results: Of 400 consecutive patients, 352 are included; the prevalence of dysphagia is 22.7%; 33 patients (9.3%) have narrowing of the sleeve with 25 (7.1%) having sharp angulation or a spiral while 8 (2.3%) have a stenosis. All 33 patients underwent balloon dilatation of the gastric sleeve and dysphagia resolved in 13 patients (39%); 10 patients (30%) noted resolution of dysphagia after two additional dilatations. In a multivariate model, medical conditions associated with post-operative dysphagia include diabetes mellitus, symptoms of esophageal reflux, a low whole blood thiamine level, hypothyroidism, use of non-steroidal anti-inflammatory drugs, and use of opioids.
Conclusion: Narrowing of the gastric sleeve and gastric sleeve stenosis are common after VSG. Endoscopic balloon dilatations of the gastric sleeve resolves dysphagia in 69% of patients.
Keywords: Bariatric surgery; Dysphagia; Obesity; Stomach dilatation; Vertical sleeve gastrectomy.
Conflict of interest statement
Conflict-of-interest statement: All of the authors have no conflict of interest to report regarding the publication of this paper.
Figures
References
-
- Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, Mullany EC, Biryukov S, Abbafati C, Abera SF, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–781. - PMC - PubMed
-
- Svetkey LP, Stevens VJ, Brantley PJ, Appel LJ, Hollis JF, Loria CM, Vollmer WM, Gullion CM, Funk K, Smith P, et al. Comparison of strategies for sustaining weight loss: the weight loss maintenance randomized controlled trial. JAMA. 2008;299:1139–1148. - PubMed
-
- Sjöström L, Narbro K, Sjöström CD, Karason K, Larsson B, Wedel H, Lystig T, Sullivan M, Bouchard C, Carlsson B, et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357:741–752. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
