

Intranasal insulin treatment of an experimental model of moderate traumatic brain injury
- PMID: 28058996
- PMCID: PMC5584695
- DOI: 10.1177/0271678X16685106
Intranasal insulin treatment of an experimental model of moderate traumatic brain injury
Abstract
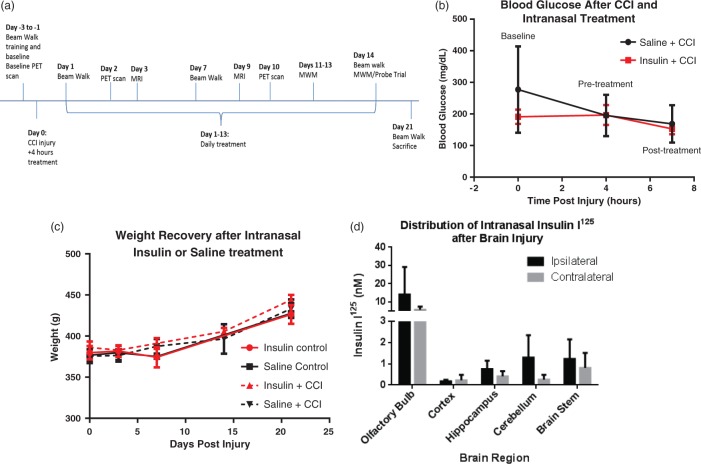
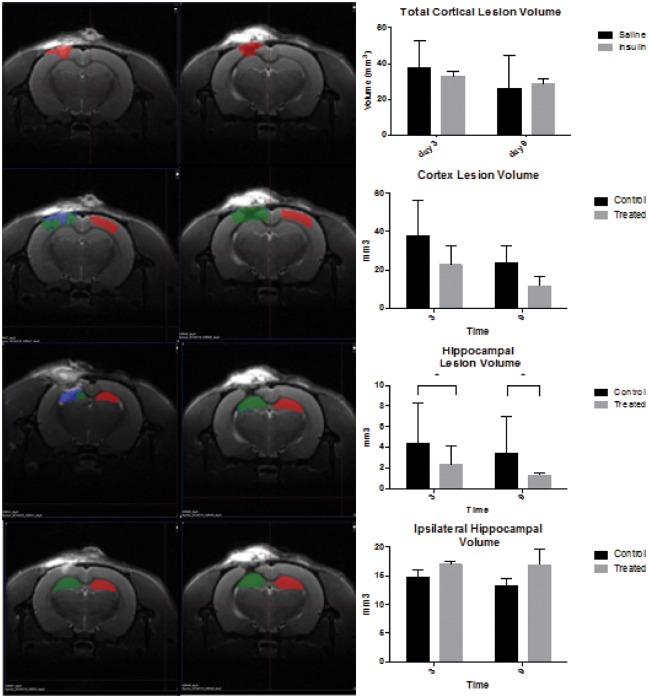
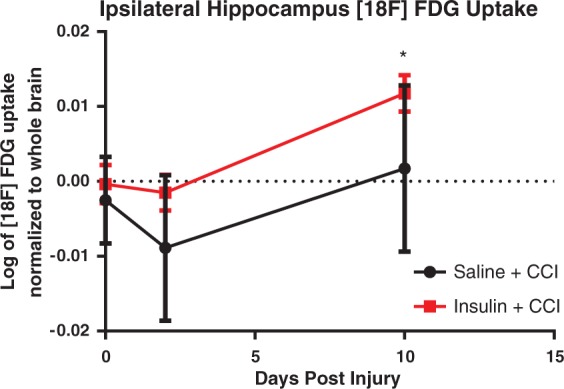
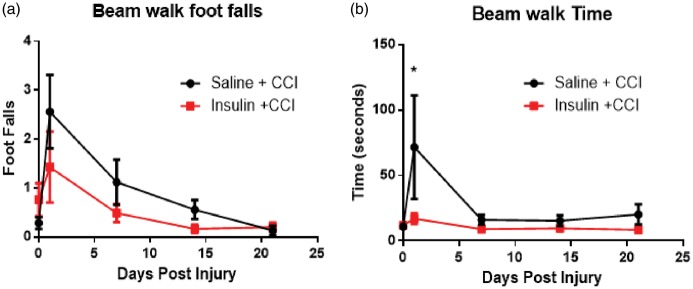
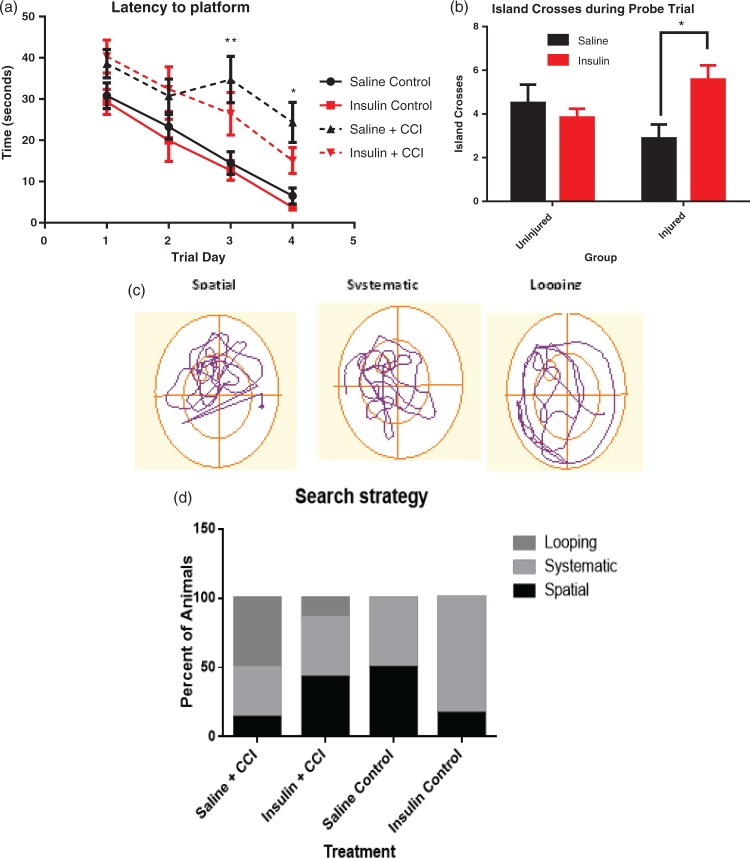
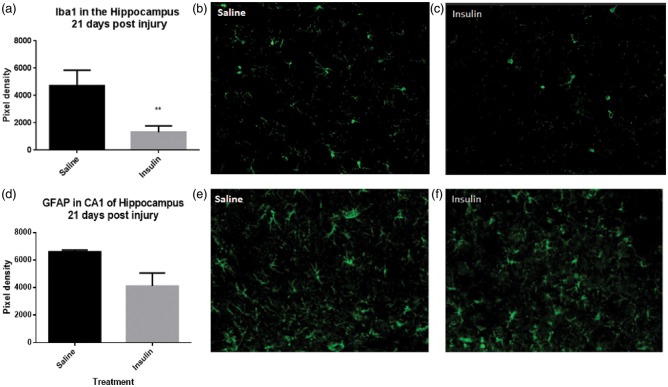
Traumatic brain injury (TBI) results in learning and memory dysfunction. Cognitive deficits result from cellular and metabolic dysfunction after injury, including decreased cerebral glucose uptake and inflammation. This study assessed the ability of intranasal insulin to increase cerebral glucose uptake after injury, reduce lesion volume, improve memory and learning function and reduce inflammation. Adult male rats received a controlled cortical impact (CCI) injury followed by intranasal insulin or saline treatment daily for 14 days. PET imaging of [18F]-FDG uptake was performed at baseline and at 48 h and 10 days post-injury and MRI on days three and nine post injury. Motor function was tested with the beam walking test. Memory function was assessed with Morris water maze. Intranasal insulin after CCI significantly improved several outcomes compared to saline. Insulin-treated animals performed better on beam walk and demonstrated significantly improved memory. A significant increase in [18F]-FDG uptake was observed in the hippocampus. Intranasal insulin also resulted in a significant decrease in hippocampus lesion volume and significantly less microglial immunolabeling in the hippocampus. These data show that intranasal insulin improves memory, increases cerebral glucose uptake and decreases neuroinflammation and hippocampal lesion volume, and may therefore be a viable therapy for TBI.
Keywords: Glucose uptake; intranasal insulin; microglia; positron emission tomography; traumatic brain injury.
Figures
References
-
- Rassovsky Y, Levi Y, Agranov E, et al. Predicting long-term outcome following traumatic brain injury (TBI). J Clin Exp Neuropsychol 2015; 37: 354–366. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
