

Safety-net Hospitals Face More Barriers Yet Use Fewer Strategies to Reduce Readmissions
- PMID: 28060053
- PMCID: PMC5309202
- DOI: 10.1097/MLR.0000000000000687
Safety-net Hospitals Face More Barriers Yet Use Fewer Strategies to Reduce Readmissions
Abstract
Objective: US hospitals that care for vulnerable populations, "safety-net hospitals" (SNHs), are more likely to incur penalties under the Hospital Readmissions Reduction Program, which penalizes hospitals with higher-than-expected readmissions. Understanding whether SNHs face unique barriers to reducing readmissions or whether they underuse readmission-prevention strategies is important.
Design: We surveyed leadership at 1600 US acute care hospitals, of whom 980 participated, between June 2013 and January 2014. Responses on 28 questions on readmission-related barriers and strategies were compared between SNHs and non-SNHs, adjusting for nonresponse and sampling strategy. We further compared responses between high-performing SNHs and low-performing SNHs.
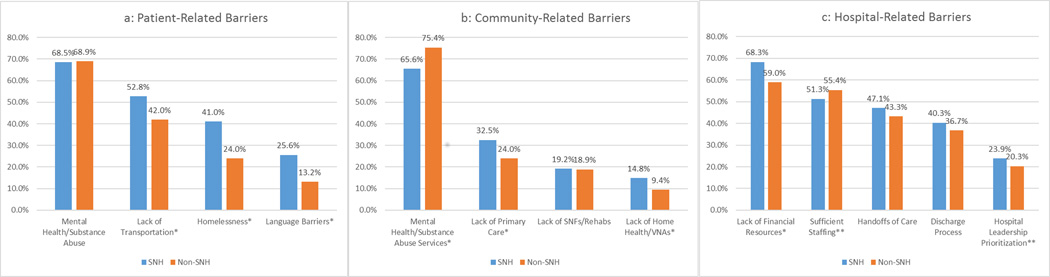
Results: We achieved a 62% response rate. SNHs were more likely to report patient-related barriers, including lack of transportation, homelessness, and language barriers compared with non-SNHs (P-values<0.001). Despite reporting more barriers, SNHs were less likely to use e-tools to share discharge summaries (70.1% vs. 73.7%, P<0.04) or verbally communicate (31.5% vs. 39.8%, P<0.001) with outpatient providers, track readmissions by race/ethnicity (23.9% vs. 28.6%, P<0.001), or enroll patients in postdischarge programs (13.3% vs. 17.2%, P<0.001). SNHs were also less likely to use discharge coordinators, pharmacists, and postdischarge programs. When we examined the use of strategies within SNHs, we found trends to suggest that high-performing SNHs were more likely to use several readmission strategies.
Conclusions: Despite reporting more barriers to reducing readmissions, SNHs were less likely to use readmission-reduction strategies. This combination of higher barriers and lower use of strategies may explain why SNHs have higher rates of readmissions and penalties under the Hospital Readmissions Reduction Program.
Conflict of interest statement
All authors do not have any conflicts of interest to disclose for the past three years.
References
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among Patients in the Medicare Fee-for-Service Program. N Engl J Med. 2009;360(14):1418–1428. - PubMed
-
- Burwell SM. Setting Value-Based Payment Goals — HHS Efforts to Improve U.S. Health Care. New England Journal of Medicine. 2015;372(10):897–899. - PubMed
-
- Rau J. Half of nation’s hospitals fail again to escape Medicare’s readmission penalties. Kaiser Health News. 2015
-
- Zuckerman RB, Sheingold SH, Orav EJ, Ruhter J, Epstein AM. Readmissions, Observation, and the Hospital Readmissions Reduction Program. New England Journal of Medicine. 2016;374(16):1543–1551. - PubMed
-
- Figueroa JF, Wang DE, Jha AK. Characteristics of hospitals receiving the largest penalties by US pay-for-performance programmes. BMJ Qual Saf. 2016 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
