

Barriers to Care and 1-Year Mortality Among Newly Diagnosed HIV-Infected People in Durban, South Africa
- PMID: 28060226
- PMCID: PMC5321110
- DOI: 10.1097/QAI.0000000000001277
Barriers to Care and 1-Year Mortality Among Newly Diagnosed HIV-Infected People in Durban, South Africa
Abstract
Background: Prompt entry into HIV care is often hindered by personal and structural barriers. Our objective was to evaluate the impact of self-perceived barriers to health care on 1-year mortality among newly diagnosed HIV-infected individuals in Durban, South Africa.
Methods: Before HIV testing at 4 outpatient sites, adults (≥18 years) were surveyed regarding perceived barriers to care including (1) service delivery, (2) financial, (3) personal health perception, (4) logistical, and (5) structural. We assessed deaths via phone calls and the South African National Population Register. We used multivariable Cox proportional hazards models to determine the association between number of perceived barriers and death within 1 year.
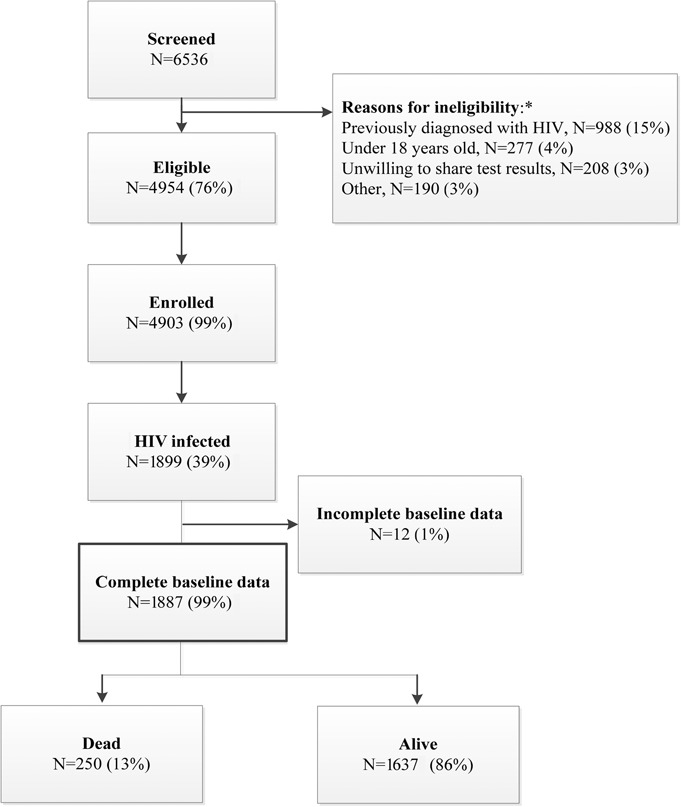
Results: One thousand eight hundred ninety-nine HIV-infected participants enrolled. Median age was 33 years (interquartile range: 27-41 years), 49% were females, and median CD4 count was 192/μL (interquartile range: 72-346/μL). One thousand fifty-seven participants (56%) reported no, 370 (20%) reported 1-3, and 460 (24%) reported >3 barriers to care. By 1 year, 250 [13%, 95% confidence interval (CI): 12% to 15%] participants died. Adjusting for age, sex, education, baseline CD4 count, distance to clinic, and tuberculosis status, participants with 1-3 barriers (adjusted hazard ratio: 1.49, 95% CI: 1.06 to 2.08) and >3 barriers (adjusted hazard ratio: 1.81, 95% CI: 1.35 to 2.43) had higher 1-year mortality risk compared with those without barriers.
Conclusions: HIV-infected individuals in South Africa who reported perceived barriers to medical care at diagnosis were more likely to die within 1 year. Targeted structural interventions, such as extended clinic hours, travel vouchers, and streamlined clinic operations, may improve linkage to care and antiretroviral therapy initiation for these people.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Mills EJ, Bakanda C, Birungi J, et al. Life expectancy of persons receiving combination antiretroviral therapy in low-income countries: a cohort analysis from Uganda. Ann Intern Med. 2011;155:209–216. - PubMed
-
- UNAIDS. South Africa HIV and AIDS Estimates. 2015. Available at: http://www.unaids.org/en/regionscountries/countries/southafrica. Accessed August 31, 2016.
-
- UNAIDS. The Gap Report. 2014. Available at: http://www.unaids.org/sites/default/files/en/media/unaids/contentassets/.... Accessed August 31, 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
