

Diagnosis of Partial Retrograde Ejaculation in Non-Azoospermic Infertile Men with Low Semen Volume
- PMID: 28060836
- PMCID: PMC5218555
- DOI: 10.1371/journal.pone.0168742
Diagnosis of Partial Retrograde Ejaculation in Non-Azoospermic Infertile Men with Low Semen Volume
Abstract
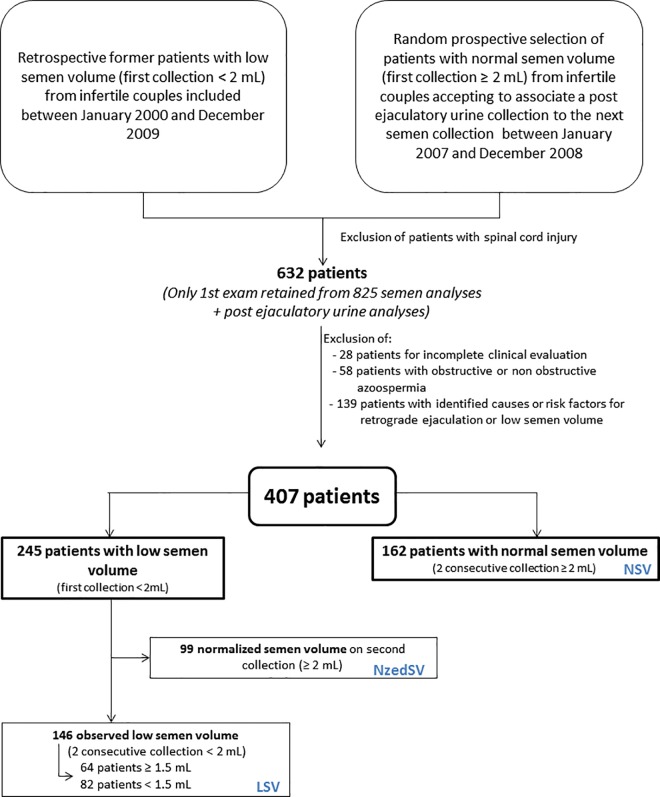
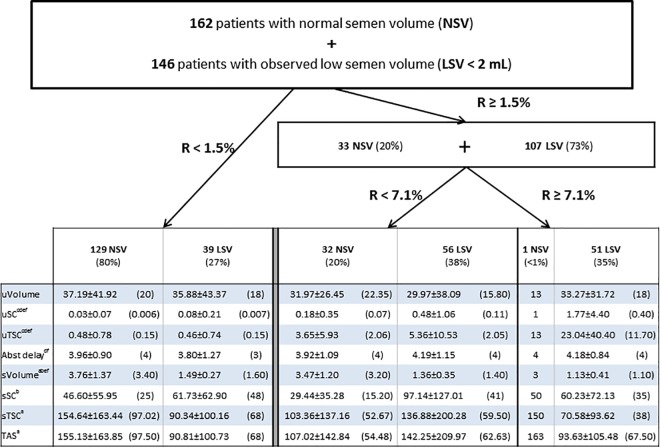
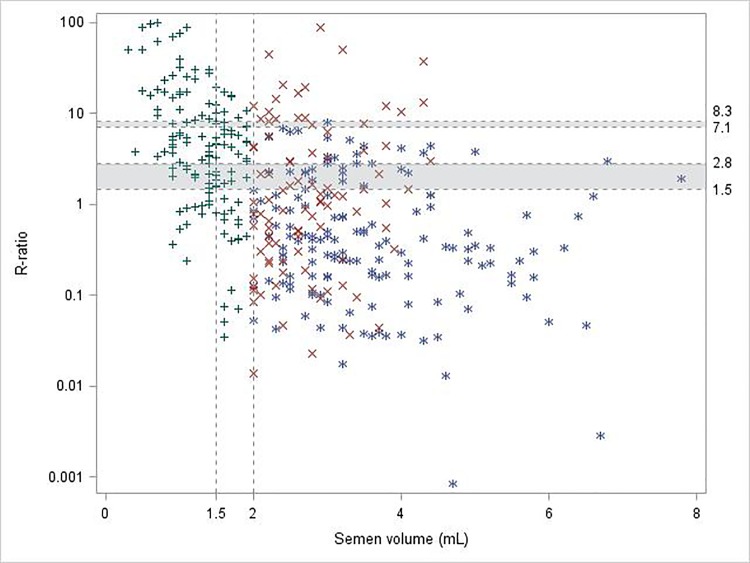
In non-azoospermic patients with low semen volume (LSV), looking for partial retrograde ejaculation (PRE) by searching sperm in the postejaculatory urine (PEU) is required. The use of a retro-ejaculatory index (R-ratio) was suggested to define PRE, but none of the studies indicated a specific threshold above which PRE must be considered. Our objective was to propose a threshold value for the R-ratio as indicative of PRE in patients with LSV selected to be devoid of any known causes or risk factors for retrograde ejaculation or LSV. Among our data base (2000-2009) including 632 patients with PEU, 245 male patients from infertile couples who had had a first semen analysis with LSV (< 2mL) and a second semen analysis associated with PEU, were selected on the previous criteria. A prospective control group was randomly constituted (2007-2008) of 162 first consulting male patients from infertile couples, with a normal semen volume (≥ 2mL) on a first semen analysis and who accepted to collect PEU with their usual second semen analysis, selected on the previous criteria. To define an R-ratio threshold indicative of PRE, we used a ROC curve analysis and a regression tree based on a classification and regression tree (CART) algorithm. Of the 245 LSV patients, 146 still presented low semen volume (< 2 mL) on the second semen analysis. From the use of the CART algorithm, two low (1.5% and 2.8%) and two high R-values (7.1% and 8.3%) were defined, according to the lower reference limit for semen volume of 2.0 mL (WHO 1999) or 1.5 mL (WHO 2010) respectively. As only one or no patient with normal semen volume was observed above the two high R-values, we suggest an R-value higher than the range of [7.1-8.3]% as indicative of PRE until confirmation by a prospective multicenter study.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Clément P, Giuliano F. Physiology and Pharmacology of Ejaculation. Basic Clin Pharmacol Toxicol. 2015 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
