

Computed Tomographic Distinction of Intimal and Medial Calcification in the Intracranial Internal Carotid Artery
- PMID: 28060941
- PMCID: PMC5218397
- DOI: 10.1371/journal.pone.0168360
Computed Tomographic Distinction of Intimal and Medial Calcification in the Intracranial Internal Carotid Artery
Abstract
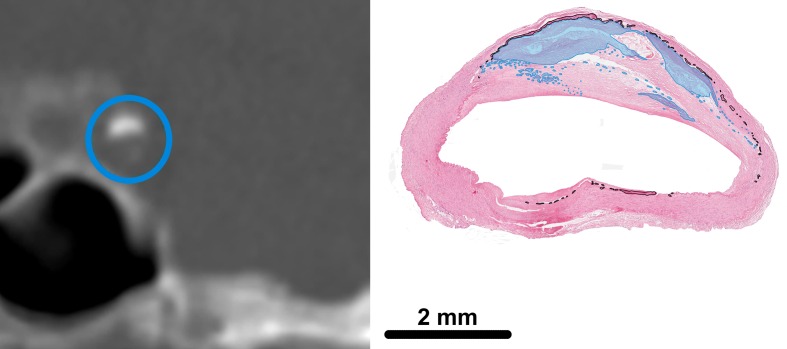
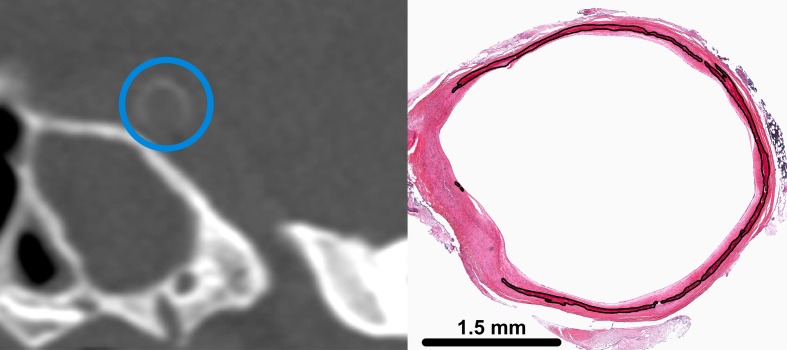
Background: Intracranial internal carotid artery (iICA) calcification is associated with stroke and is often seen as a proxy of atherosclerosis of the intima. However, it was recently shown that these calcifications are predominantly located in the tunica media and internal elastic lamina (medial calcification). Intimal and medial calcifications are thought to have a different pathogenesis and clinical consequences and can only be distinguished through ex vivo histological analysis. Therefore, our aim was to develop CT scoring method to distinguish intimal and medial iICA calcification in vivo.
Methods: First, in both iICAs of 16 cerebral autopsy patients the intimal and/or medial calcification area was histologically assessed (142 slides). Brain CT images of these patients were matched to the corresponding histological slides to develop a CT score that determines intimal or medial calcification dominance. Second, performance of the CT score was assessed in these 16 patients. Third, reproducibility was tested in a separate cohort.
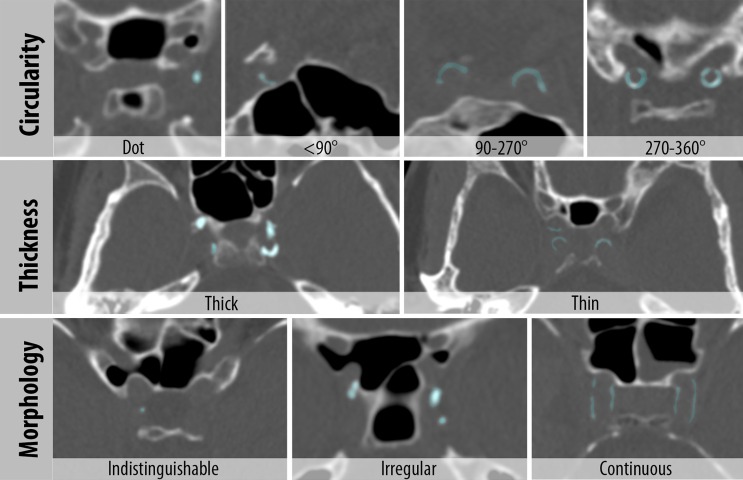
Results: First, CT features of the score were circularity (absent, dot(s), <90°, 90-270° or 270-360°), thickness (absent, ≥1.5mm, or <1.5mm), and morphology (indistinguishable, irregular/patchy or continuous). A high sum of features represented medial and a lower sum intimal calcifications. Second, in the 16 patients the concordance between the CT score and the dominant calcification type was reasonable. Third, the score showed good reproducibility (kappa: 0.72 proportion of agreement: 0.82) between the categories intimal, medial or absent/indistinguishable.
Conclusions: The developed CT score shows good reproducibility and can differentiate reasonably well between intimal and medial calcification dominance in the iICA, allowing for further (epidemiological) studies on iICA calcification.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Erbay S, Han R, Baccei S, Krakov W, Zou KH, Bhadelia R, et al. Intracranial carotid artery calcification on head CT and its association with ischemic changes on brain MRI in patients presenting with stroke-like symptoms: Retrospective analysis. Neuroradiology. 2007;49:27–33. 10.1007/s00234-006-0159-z - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
