

Moebius sequence -a multidisciplinary clinical approach
- PMID: 28061881
- PMCID: PMC5217236
- DOI: 10.1186/s13023-016-0559-z
Moebius sequence -a multidisciplinary clinical approach
Abstract
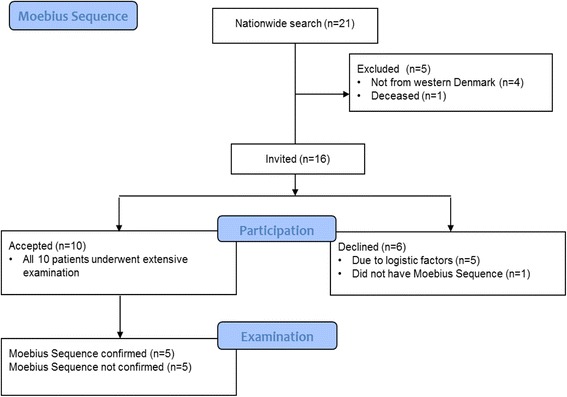
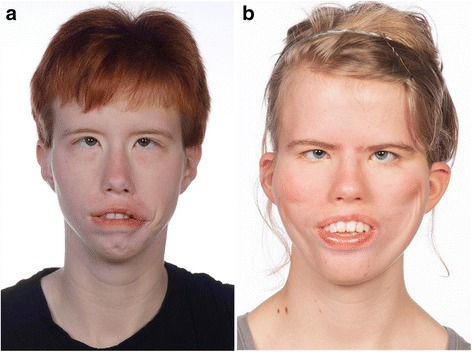
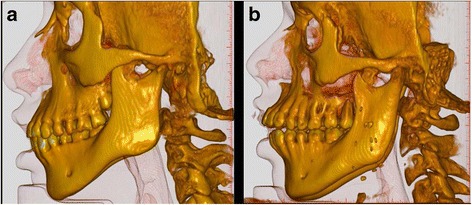
Background: Moebius Sequence (MS) is a rare disorder defined by bilateral congenital paralysis of the abducens and facial nerves in combination with various odontological, craniofacial, ophthalmological and orthopaedic conditions. The aetiology is still unknown; but both genetic (de novo mutations) and vascular events in utero are reported. The purpose of present study was through a multidisciplinary clinical approach to examine children diagnosed with Moebius-like symptoms. Ten children underwent odontological, ophthalmological, obstetric, paediatric, orthopaedic, genetic, radiological and photographical evaluation. Five patients maintained the diagnosis of MS according to the diagnostic criteria.
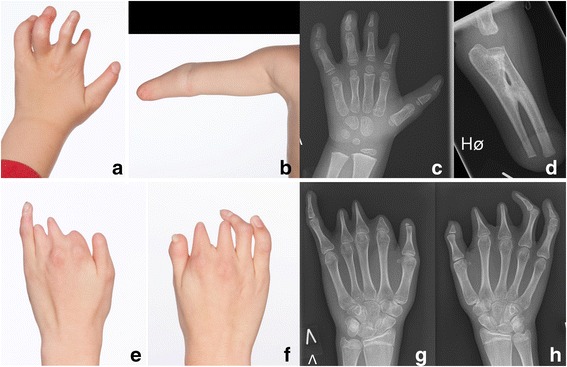
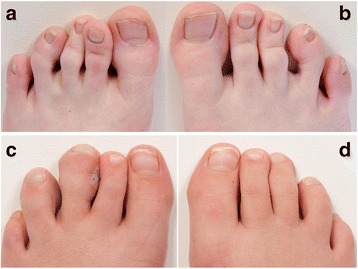
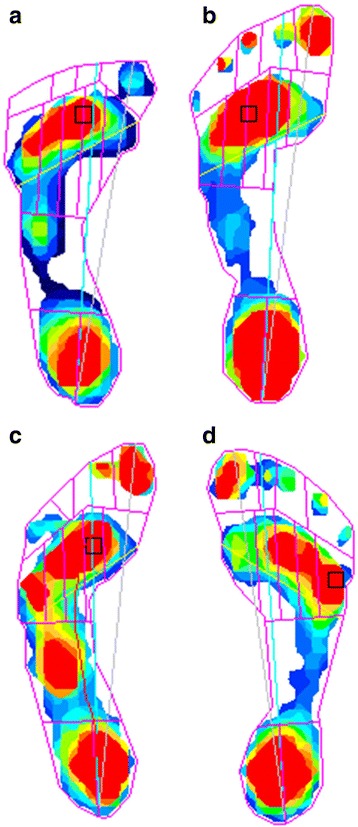
Results: All five patients had bilateral facial and abducens paralysis confirmed by ophthalmological examination. Three of five had normal brain MR imaging. Two had missing facial nerves and one had missing abducens nerves. The Strengths and Difficulties Questionnaire (SDQ) showed normal scores in three of five patients. Interestingly, two of five children were born to mothers with uterine abnormalities (unicornuate/bicornuate uterus). In the odontological examination three of five showed enamel hypomineralisation. All five had abnormal orofacial motor function and maxillary prognathism. Two patients had adactyly, syndactyly and brachydactyly. None of the five patients had Poland anomaly, hip dislocation or dysplasia but all had a mild degree of scoliosis. We observed congenital club-feet, calcaneovalgus deformities, macrodactyly of one or more toes or curly toes. Pedobarography showed plantar pressures within normal ranges.
Conclusions: Adherence to standard diagnostic criteria is central in the diagnosis of MS. An accurate diagnosis is the basis for correct discussion of other relevant concomitant symptoms of MS, genetic testing and evaluation of prognosis. The multidisciplinary approach and adherence to diagnostic criteria taken in present study increases the knowledge on the relationship between genotype, phenotype and symptomatology of MS.
Keywords: Children; Moebius Sequence; Multidisciplinary Approach; Rare Disease.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
