

Evolution in the utilization of biliary interventions in the United States: results of a nationwide longitudinal study from 1998 to 2013
- PMID: 28062313
- PMCID: PMC5496794
- DOI: 10.1016/j.gie.2016.12.021
Evolution in the utilization of biliary interventions in the United States: results of a nationwide longitudinal study from 1998 to 2013
Abstract
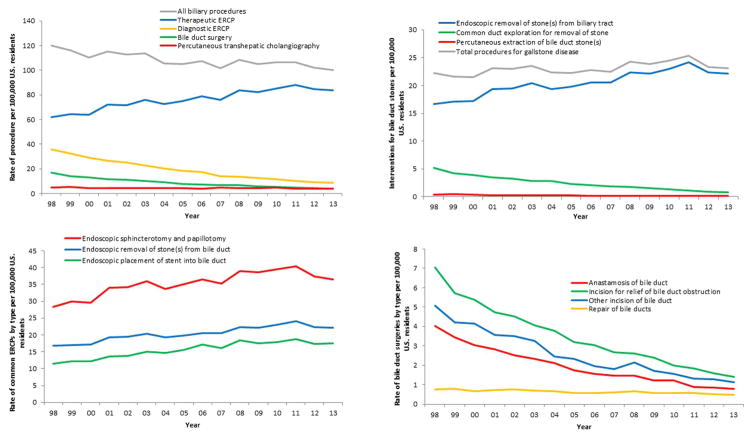
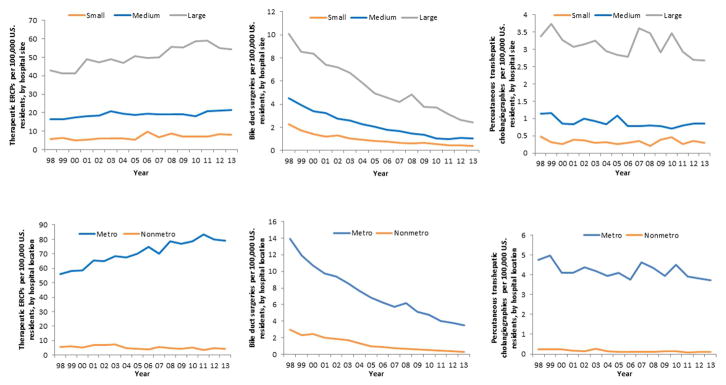
Background and aims: Bile duct surgery (BDS), percutaneous transhepatic cholangiography (PTC), and ERCP are alternative interventions used to treat biliary disease. Our aim was to describe trends in ERCP, BDS, and PTC on a nationwide level in the United States.
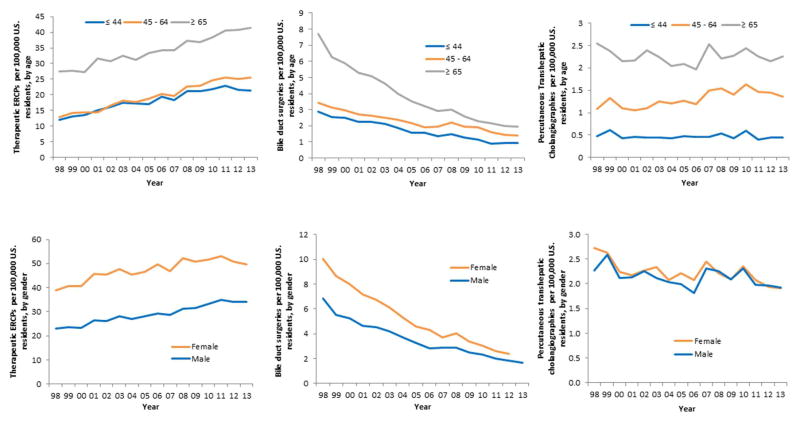
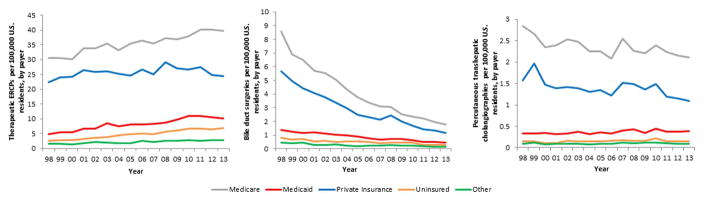
Methods: We used the National Inpatient Sample to estimate age-standardized utilization trends of inpatient diagnostic ERCP, therapeutic ERCP, BDS, and PTC between 1998 and 2013. We calculated average case fatality, length of stay, patient demographic profile (age, gender, payer), and hospital characteristics (hospital size and metropolitan status) for these procedures.
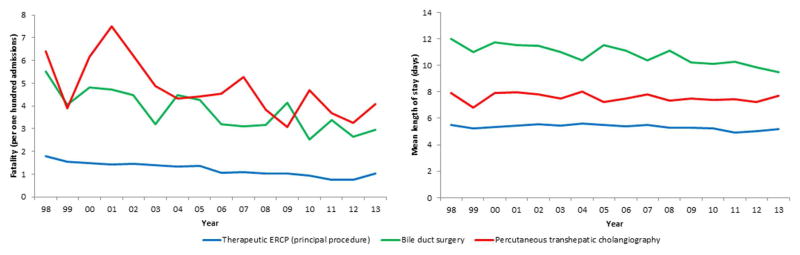
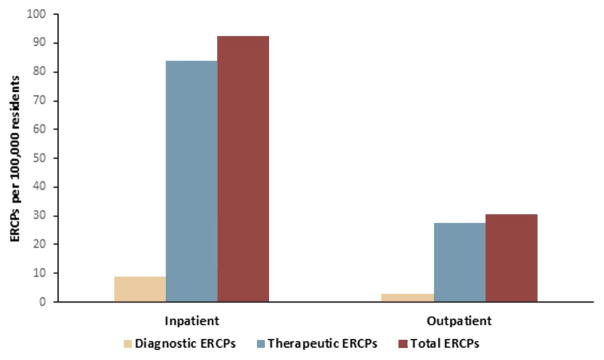
Results: Total biliary interventions decreased over the study period from 119.8 to 100.1 per 100,000. Diagnostic ERCP utilization decreased by 76%, and therapeutic ERCP utilization increased by 35%. BDS rates decreased by 78% and PTC rates by 24%. ERCP has almost completely supplanted surgery for the management of choledocholithiasis. Fatality from ERCP, BDS, and PTC have all decreased, whereas mean length of stay has remained stable. The proportion of Medicare-insured, Medicaid-insured, and uninsured patients undergoing biliary procedures has increased over time. Most of the increase in therapeutic ERCP and decrease in BDS occurred in large, metropolitan hospitals.
Conclusions: Although therapeutic ERCP utilization has increased over time, the total volume of biliary interventions has decreased. BDS utilization has experienced the most dramatic decrease, possibly a consequence of the increased therapeutic capacity and safety of ERCP. ERCPs are now predominantly therapeutic in nature. Large urban hospitals are leading the shift from surgical to endoscopic therapy of the biliary system.
Copyright © 2017 American Society for Gastrointestinal Endoscopy. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Fifteen years of ERCP.Gastrointest Endosc. 2017 Aug;86(2):327-328. doi: 10.1016/j.gie.2017.03.1547. Gastrointest Endosc. 2017. PMID: 28728670 No abstract available.
References
-
- Ogoshi K, Tobita Y, Hara Y. Endoscopic observation of the duodenum and pancreatocholedochography using duodenofiberscope under direct vision. Gastrointestinal Endoscopy. 1970;12:83–96.
-
- Takagi K, Ikeda S, Nakagawa Y, et al. Retrograde pancreatography and cholangiography by fiber duodenoscope. Gastroenterology. 1970;59:445–52. - PubMed
-
- Kawai K, Akasaka Y, Murakami K, et al. Endoscopic sphincterotomy of the ampulla of Vater. Gastrointest Endosc. 1974;20:148–51. - PubMed
-
- Cotton PB, Chapman M, Whiteside CG, et al. Duodenoscopic papillotomy and gallstone removal. Br J Surg. 1976;63:709–14. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
