

Lipoprotein(a) Mass Levels Increase Significantly According to APOE Genotype: An Analysis of 431 239 Patients
- PMID: 28062489
- PMCID: PMC5323356
- DOI: 10.1161/ATVBAHA.116.308704
Lipoprotein(a) Mass Levels Increase Significantly According to APOE Genotype: An Analysis of 431 239 Patients
Abstract
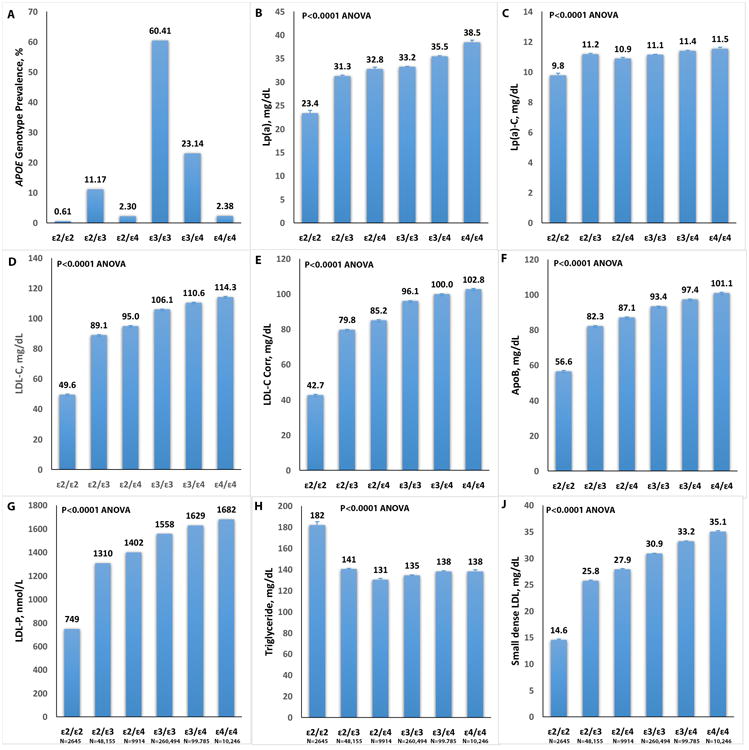
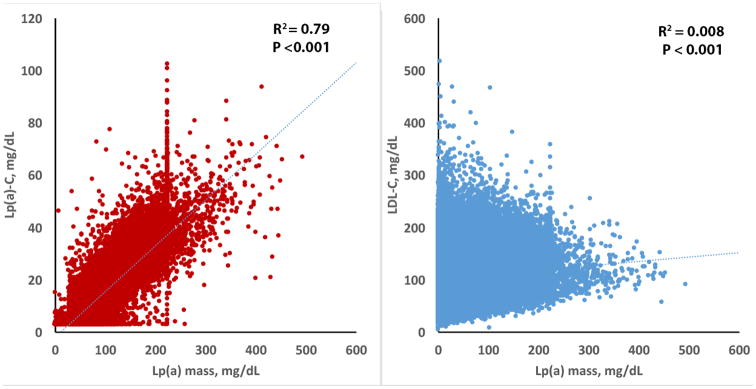
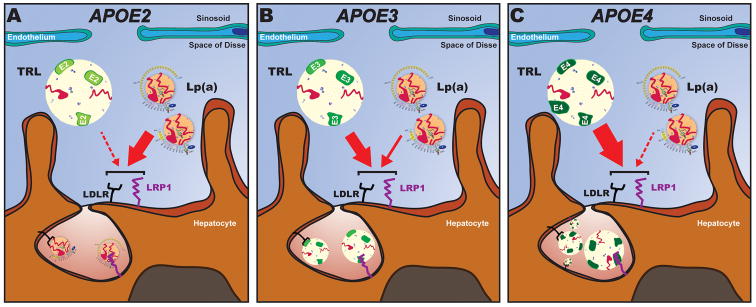
Objective: Lipoprotein(a) [Lp(a)] levels are genetically determined by hepatocyte apolipoprotein(a) synthesis, but catabolic pathways also influence circulating levels. APOE genotypes have different affinities for the low-density lipoprotein (LDL) receptor and LDL-related protein-1, with ε2 having the weakest binding to LDL receptor at <2% relative to ε3 and ε4. APPROACH AND RESULTS: APOE genotypes (ε2/ε2, ε2/ε3, ε2/ε4, ε3/ε3, ε3/ε4, and ε4/ε4), Lp(a) mass, directly measured Lp(a)-cholesterol levels, and a variety of apoB-related lipoproteins were measured in 431 239 patients. The prevalence of APOE traits were ε2: 7.35%, ε3: 77.56%, and ε4: 15.09%. Mean (SD) Lp(a) levels were 65% higher in ε4/ε4 compared with ε2/ε2 genotypes and increased significantly according to APOE genotype: ε2/ε2: 23.4 (29.2), ε2/ε3: 31.3 (38.0), ε2/ε4: 32.8 (38.5), ε3/ε3: 33.2 (39.1), ε3/ε4: 35.5 (41.6), and ε4/ε4: 38.5 (44.1) mg/dL (P<0.0001). LDL-cholesterol, apoB, Lp(a)-cholesterol, LDL-cholesterol corrected for Lp(a)-cholesterol content, LDL-particle number, and small, dense LDL also had similar patterns. Patients with LDL-cholesterol ≥250 mg/dL, who are more likely to have LDL receptor mutations and reduced affinity for apoB, had higher Lp(a) levels across all apoE isoforms, but particularly in patients with ε2 alleles, compared with LDL <250 mg/dL. The lowest Lp(a) mass levels were present in patients with ε2 isoforms and lowest LDL-cholesterol.
Conclusions: APOE genotypes strongly influence Lp(a) and apoB-related lipoprotein levels. This suggests that differences in affinity of apoE proteins for lipoprotein clearance receptors may affect Lp(a) catabolism, suggesting a competition between Lp(a) and apoE protein for similar receptors.
Keywords: alleles; cholesterol; genotype; hepatocytes; prevalence.
© 2017 American Heart Association, Inc.
Figures
References
-
- Capoulade R, Chan KL, Yeang C, Mathieu P, Bosse Y, Dumesnil JG, Tam JW, Teo KK, Mahmut A, Yang X, Witztum JL, Arsenault BJ, Despres JP, Pibarot P, Tsimikas S. Oxidized phospholipids, lipoprotein(a), and progression of calcific aortic valve stenosis. J Am Coll Cardiol. 2015;66:1236–1246. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
