

White Matter Hyperintensity Associations with Cerebral Blood Flow in Elderly Subjects Stratified by Cerebrovascular Risk
- PMID: 28063772
- PMCID: PMC5473621
- DOI: 10.1016/j.jstrokecerebrovasdis.2016.10.017
White Matter Hyperintensity Associations with Cerebral Blood Flow in Elderly Subjects Stratified by Cerebrovascular Risk
Abstract
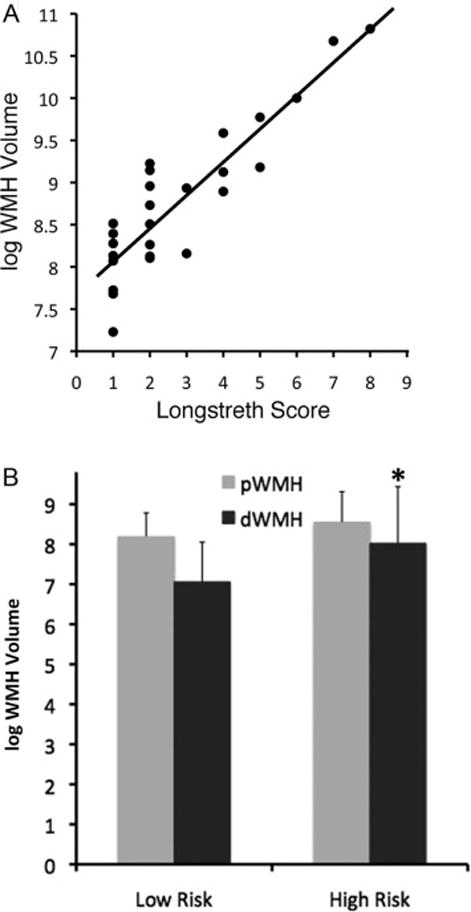
Objective: This study aims to add clarity to the relationship between deep and periventricular brain white matter hyperintensities (WMHs), cerebral blood flow (CBF), and cerebrovascular risk in older persons.
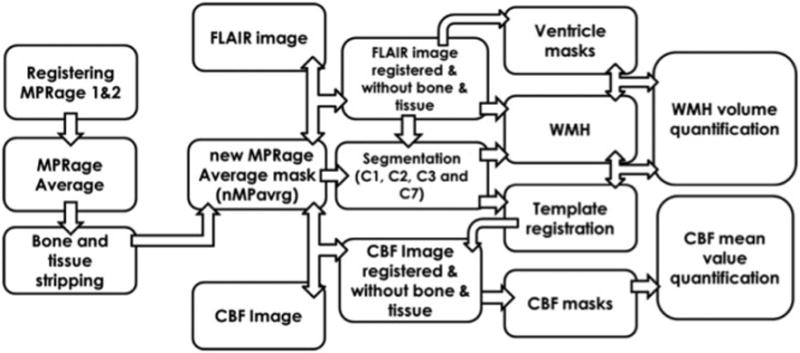
Methods: Deep white matter hyperintensity (dWMH) and periventricular white matter hyperintensity (pWMH) and regional gray matter (GM) and white matter (WM) blood flow from arterial spin labeling were quantified from magnetic resonance imaging scans of 26 cognitively normal elderly subjects stratified by cerebrovascular disease (CVD) risk. Fluid-attenuated inversion recovery images were acquired using a high-resolution 3-dimensional (3-D) sequence that reduced partial volume effects seen with slice-based techniques.
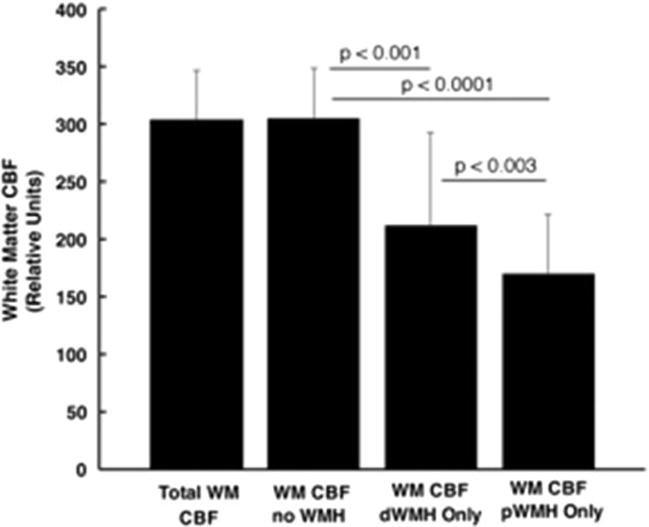
Results: dWMHs but not pWMHs were increased in patients at high risk of CVD; pWMHs but not dWMHs were associated with decreased regional cortical (GM) blood flow. We also found that blood flow in WM is decreased in regions of both pWMH and dWMH, with a greater degree of decrease in pWMH areas.
Conclusions: WMHs are usefully divided into dWMH and pWMH regions because they demonstrate differential effects. 3-D regional WMH volume is a potentially valuable marker for CVD based on associations with cortical CBF and WM CBF.
Keywords: White matter hyperintensities; arterial spin-labeling image; cerebral blood flow; fluid-attenuated inversion recovery; segmentation; small-vessel disease; vascular risk.
Copyright © 2017 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Jellinger KA. The pathology of ischemic-vascular dementia: an update. Journal of the neurological sciences. 2002:203–204. 153–7. - PubMed
-
- Gootjes L, Teipel SJ, Zebuhr Y, Schwarz R, Leinsinger G, Scheltens P, et al. Regional distribution of white matter hyperintensities in vascular dementia, Alzheimer's disease and healthy aging. Dementia and geriatric cognitive disorders. 2004;18:180–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
