

Effect of immediate initiation of antiretroviral therapy on risk of severe bacterial infections in HIV-positive people with CD4 cell counts of more than 500 cells per μL: secondary outcome results from a randomised controlled trial
- PMID: 28063815
- PMCID: PMC5337625
- DOI: 10.1016/S2352-3018(16)30216-8
Effect of immediate initiation of antiretroviral therapy on risk of severe bacterial infections in HIV-positive people with CD4 cell counts of more than 500 cells per μL: secondary outcome results from a randomised controlled trial
Abstract
Background: The effects of antiretroviral therapy on risk of severe bacterial infections in people with high CD4 cell counts have not been well described. In this study, we aimed to quantify the effects of immediate versus deferred ART on the risk of severe bacterial infection in people with high CD4 cell counts in a preplanned analysis of the START trial.
Methods: The START trial was a randomised controlled trial in ART-naive HIV-positive patients with CD4 cell count of more than 500 cells per μL assigned to immediate ART or deferral until their CD4 cell counts were lower than 350 cells per μL. We used Cox proportional hazards regression to model time to severe bacterial infection, which was defined as a composite endpoint of bacterial pneumonia (confirmed by the endpoint review committee), pulmonary or extrapulmonary tuberculosis, or any bacterial infectious disorder of grade 4 severity, that required unscheduled hospital admissions, or caused death. This study is registered with ClinicalTrials.gov, number NCT00867048.
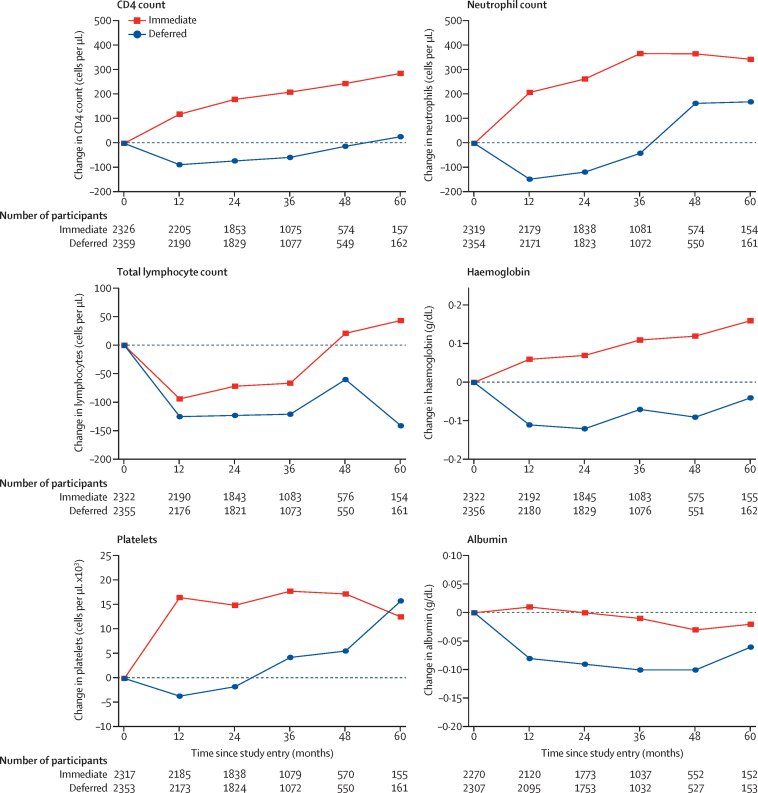
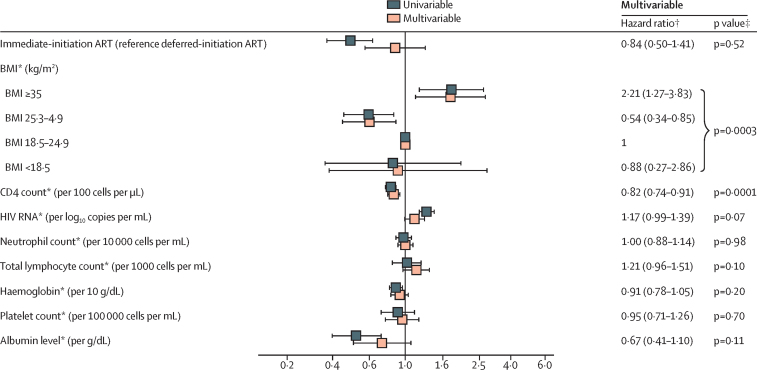
Findings: Patients were recruited from April 15, 2009, to Dec 23, 2013. The data cutoff for follow-up was May 26, 2015. Of 4685 HIV-positive people enrolled, 120 had severe bacterial infections (immediate-initiation group n=34, deferred-initiation group n=86; median 2·8 years of follow-up). Immediate ART was associated with a reduced risk of severe bacterial infection compared with deferred ART (hazard ratio [HR] 0·39, 95% CI 0·26-0·57, p<0·0001). In the immediate-initiation group, average neutrophil count over follow-up was 321 cells per μL higher, and average CD4 cell count 194 cells per μL higher than the deferred-initiation group (p<0·0001). In univariable analysis, higher time-updated CD4 cell count (0·78, 0·71-0·85, p=0·0001) was associated with reduced risk of severe bacterial infection. Time-updated neutrophil count was not associated with severe bacterial infection. After adjustment for time-updated factors in multivariable analysis, particularly the CD4 cell count, the HR for immediate-initiation group moved closer to 1 (HR 0·84, 0·50-1·41, p=0·52). These results were consistent when subgroups of the severe bacterial infection composite were analysed separately.
Interpretation: Immediate ART reduces the risk of several severe bacterial infections in HIV-positive people with high CD4 cell count. This is partly explained by ART-induced increases in CD4 cell count, but not by increases in neutrophil count.
Funding: National Institute of Allergy and Infectious Diseases National Institutes of Health, Agence Nationale de Recherches sur le SIDA et les Hépatites Virales, Bundesministerium für Bildung und Forschung, European AIDS Treatment Network, Australian National Health and Medical Research Council, UK National Institute for Health Research and Medical Research Council, Danish National Research Foundation.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Severe bacterial infections: overlooked opportunistic diseases.Lancet HIV. 2017 Mar;4(3):e94-e95. doi: 10.1016/S2352-3018(16)30213-2. Epub 2017 Jan 5. Lancet HIV. 2017. PMID: 28063814 No abstract available.
References
-
- British HIV Association British HIV Association guidelines for the treatment of HIV-1-positive adults with antiretroviral therapy. 2015. http://www.bhiva.org/documents/Guidelines/Treatment/2015/2015-treatment-... (accessed Nov 3, 2015). - PubMed
-
- European AIDS Clinical Society Guidelines version 8.0. October, 2015. http://www.eacsociety.org/files/2015_eacsguidelines_8.0-english_revised-... (accessed Nov 3, 2015).
-
- WHO Guidelines on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV. September, 2015. http://apps.who.int/iris/bitstream/10665/186275/1/9789241509565_eng.pdf (accessed Nov 3, 2015). - PubMed
-
- Anglaret X, Messou E, Ouassa T. Pattern of bacterial diseases in a cohort of HIV-1 infected adults receiving cotrimoxazole prophylaxis in Abidjan, Cote D'Ivoire. AIDS. 2003;17:575–584. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
