

Arteriovenous Grafts: Much Maligned But in Need of Reconsideration?
- PMID: 28064472
- PMCID: PMC5334188
- DOI: 10.1111/sdi.12567
Arteriovenous Grafts: Much Maligned But in Need of Reconsideration?
Abstract
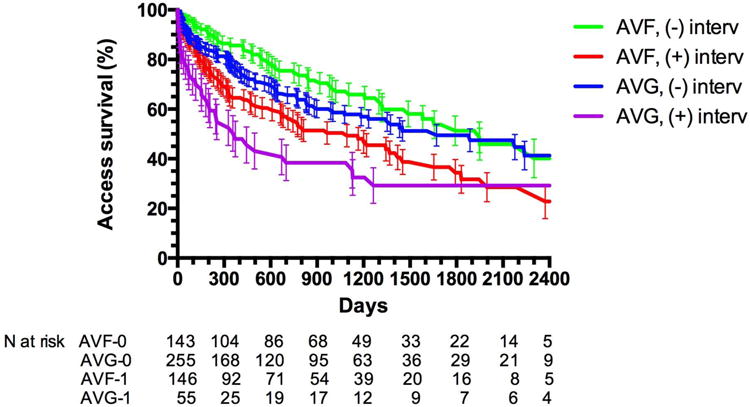
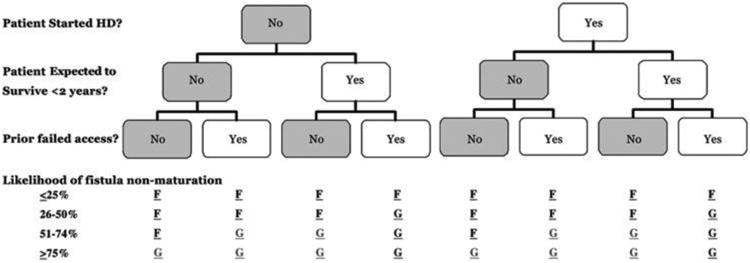
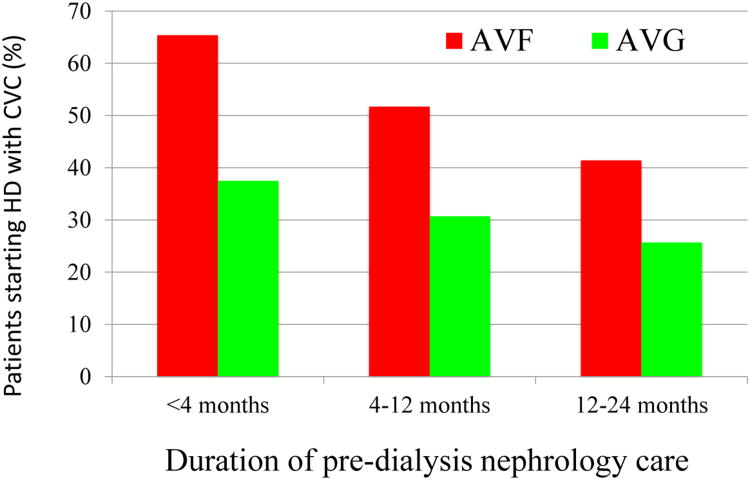
There are substantial variations in arteriovenous fistula (AVF) use among hemodialysis patients in different countries, in different regions of the U.S., and even in different hemodialysis units within a single metropolitan area. These variations persist after adjustment for patient demographics and comorbidities, suggesting that practice patterns play a major role in determining the frequency of AVF use. These observations led to vascular access guidelines urging nephrologists and surgeons to increase AVF creation in patients with chronic kidney disease. Over the past 20 years, as clinicians have adopted these guidelines, the prevalence of AVF use in hemodialysis patients has increased substantially. At the same time, clinicians have recognized important limitations of an unwavering "Fistula First" approach. First, a substantial proportion of AVFs fail to mature even when routine preoperative vascular mapping is used, leading to prolonged catheter dependence. Second, certain patient subgroups are at high risk for AVF nonmaturation. Third, nonmaturing AVFs frequently require interventions to promote their maturation. Fourth, AVFs that require such interventions have shortened cumulative patency. Fifth, arteriovenous grafts (AVG) have several advantages over AVFs, including lower primary failure rates, fewer interventions prior to successful cannulation, and shorter duration of catheter dependence with its associated risk of bacteremia. All these observations have led nephrologists to propose an individualized approach to vascular access, with AVG being preferred in patients who initiate hemodialysis with a catheter, particularly if they are at high risk for AVF nonmaturation and have a relatively short life expectancy.
© 2017 Wiley Periodicals, Inc.
Figures
References
-
- Hirth RA, Turenne MN, Woods JD, Young EW, Port FK, Pauly MV, et al. Predictors of type of vascular access in hemodialysis patients. JAMA. 1996;276:1303–07. - PubMed
-
- Allon M, Ornt D, Schwab S, Rasmussen C, Delmez JA, Greene T, et al. Factors associated with the prevalence of A-V fistulas in hemodialysis patients in the HEMO Study. Kidney Int. 2000;58:2178–85. - PubMed
-
- Pisoni RL, Young EW, Dykstra DM, Greenwood RN, Hecking E, Gillespie B, et al. Vascular access use in Europe and in the United States: Results from the DOPPS. Kidney Int. 2002;61:305–16. - PubMed
-
- Rayner HC, Pisoni Rl, Gillespie BW, Goodkin DA, Akiba T, Azikawa T, et al. Creation, cannulation, and survival of arteriovenous fistulae: Data from the Dialysis Outcomes and Practice Patterns Study. Kidney Int. 2003;63:323–30. - PubMed
-
- NKF-DOQI Clinical Practice Guidelines for Vascular Access. New York: National Kidney Foundation; 1997. pp. 22–23. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
