

The predictive capabilities of a novel cardiovascular magnetic resonance derived marker of cardiopulmonary reserve on established prognostic surrogate markers in patients with pulmonary vascular disease: results of a longitudinal pilot study
- PMID: 28065166
- PMCID: PMC5220614
- DOI: 10.1186/s12968-016-0316-4
The predictive capabilities of a novel cardiovascular magnetic resonance derived marker of cardiopulmonary reserve on established prognostic surrogate markers in patients with pulmonary vascular disease: results of a longitudinal pilot study
Abstract
Background: No unified method exists to effectively predict and monitor progression of pulmonary arterial hypertension (PAH). We assessed the longitudinal relationship between a novel marker of cardiopulmonary reserve and established prognostic surrogate markers in patients with pulmonary vascular disease.
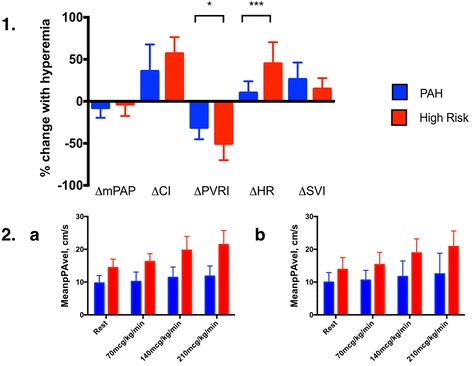
Methods and results: Twenty participants with confirmed (n = 14) or at high risk (n = 6) for PAH underwent cardiovascular magnetic resonance (CMR) at baseline and after ~6 months of guideline-appropriate management. Ten PAH participants underwent RHC within 48 h of each CMR. RHC (mean pulmonary arterial pressure, mPAP; pulmonary vascular resistance index, PVRI; cardiac index, CI) and phase-contrast CMR (mean pulmonary arterial blood flow velocity, meanPAvel) measurements were taken at rest and during continuous adenosine infusion (70/140/210 mcg/kg/min). Initial meanPAvel's (rest and hyperemic) were correlated with validated surrogate prognostic parameters (CMR: RV ejection fraction, RVEF; RV end systolic volume indexed, RVESVI; RHC: PVRI, CI; biomarker: NT-pro brain natriuretic peptide, NTpBNP; clinical: 6-min walk distance, 6MWD), a measure of pulmonary arterial stiffness (elastic modulus) and volumetric estimation of RV ventriculoarterial (VA) coupling. Changes in meanPAvel's were correlated with changes in comparator parameters over time. At initial assessment, meanPAvel at rest correlated significantly with PVRI (inversely), CI (positively) and elastic modulus (inversely) (R 2 > 0.37,P < 0.05 for all), whereas meanPAvel at peak hyperemia correlated significantly with PVRI, RVEF, RVESVI, 6MWD, elastic modulus and VA coupling (R 2 > 0.30,P < 0.05 for all). Neither resting or hyperemia-derived meanPAvel correlated with NTpBNP levels. Initial meanPAvel at rest correlated significantly with RVEF, RVESVI, CI and VA coupling at follow up assessment (R 2 > 0.2,P < 0.05 for all) and initial meanPAvel at peak hyperemia correlated with RVEF, RVESVI, PVRI and VA coupling (R 2 > 0.37,P < 0.05 for all). Change in meanPAvel at rest over time did not show statistically significant correlation with change in prognostic parameters, while change in meanPAvel at peak hyperemia did show a significant relationship with ΔRVEF, ΔRVESVI, ΔNTpBNP and ΔCI (R 2 > 0.24,P < 0.05 for all).
Conclusion: MeanPAvel during peak hyperemia correlated with invasive, non-invasive and clinical prognostic parameters at different time points. Further studies with predefined clinical endpoints are required to evaluated if this novel tool is a marker of disease progression in patients with pulmonary vascular disease.
Figures


References
-
- Baillie TJ, S; Steele, PM; Worthley SG; Willoughby, S; Teo, K; Sanders, P; Nicholls SJ; Worthley MI. Non-invasive assessment of cardiopulmonary reserve: towards early detection of pulmonary vascular disease. American journal of respiratory and critical care medicine. IN PRESS 2016. - PubMed
-
- Galie N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, Beghetti M, Corris P, Gaine S, Gibbs JS, Gomez-Sanchez MA, Jondeau G, Klepetko W, Opitz C, Peacock A, Rubin L, Zellweger M, Simonneau G. Guidelines for the diagnosis and treatment of pulmonary hypertension: the task force for the diagnosis and treatment of pulmonary hypertension of the European society of cardiology (ESC) and the European respiratory society (ERS), endorsed by the international society of heart and lung transplantation (ISHLT) Eur Heart J. 2009;30:2493–2537. doi: 10.1093/eurheartj/ehp297. - DOI - PubMed
-
- Galie N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, Simonneau G, Peacock A, Vonk Noordegraaf A, Beghetti M, Ghofrani A, Gomez Sanchez MA, Hansmann G, Klepetko W, Lancellotti P, Matucci M, McDonagh T, Pierard LA, Trindade PT, Zompatori M, Hoeper M, Aboyans V, Vaz Carneiro A, Achenbach S, Agewall S, Allanore Y, Asteggiano R, Paolo Badano L, Albert Barbera J, Bouvaist H, Bueno H, Byrne RA, Carerj S, Castro G, Erol C, Falk V, Funck-Brentano C, Gorenflo M, Granton J, Iung B, Kiely DG, Kirchhof P, Kjellstrom B, Landmesser U, Lekakis J, Lionis C, Lip GY, Orfanos SE, Park MH, Piepoli MF, Ponikowski P, Revel MP, Rigau D, Rosenkranz S, Voller H, Zamorano LJ. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: the joint task force for the diagnosis and treatment of pulmonary hypertension of the European society of cardiology (ESC) and the European respiratory society (ERS): endorsed by: association for European paediatric and congenital cardiology (AEPC), international society for heart and lung transplantation (ISHLT) Eur Heart J. 2016;37:67–119. doi: 10.1093/eurheartj/ehv317. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
