

Techniques of stapler-based navigational thoracoscopic segmentectomy using virtual assisted lung mapping (VAL-MAP)
- PMID: 28066675
- PMCID: PMC5179343
- DOI: 10.21037/jtd.2016.09.56
Techniques of stapler-based navigational thoracoscopic segmentectomy using virtual assisted lung mapping (VAL-MAP)
Abstract
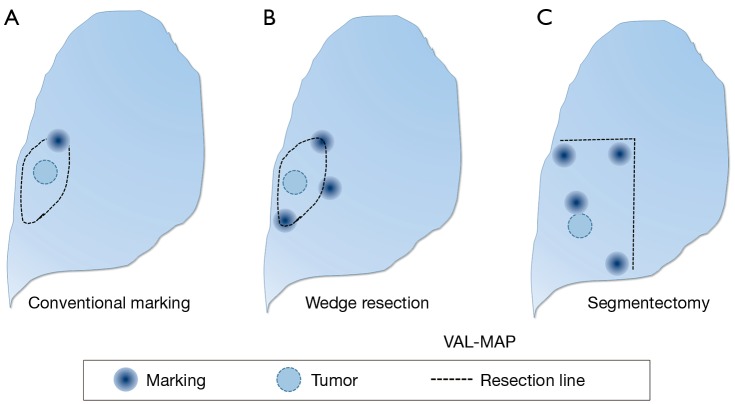
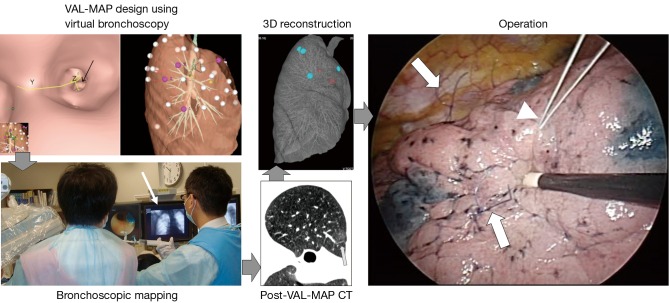
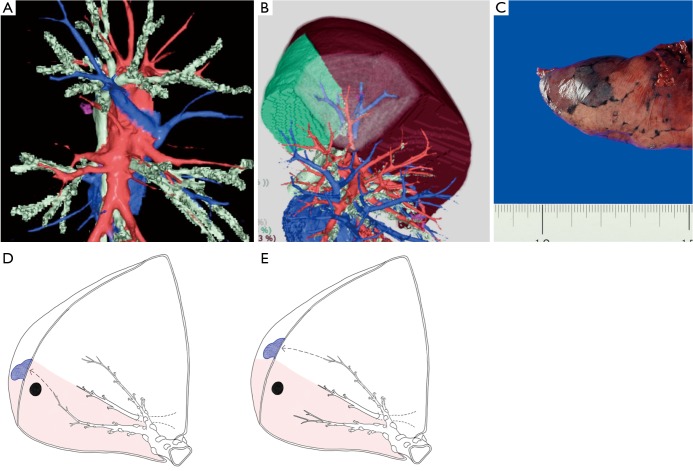
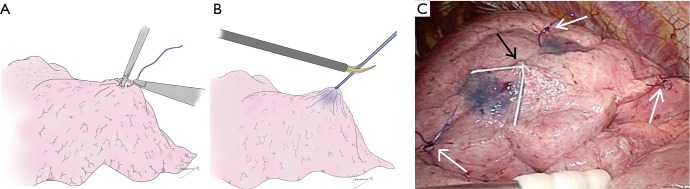
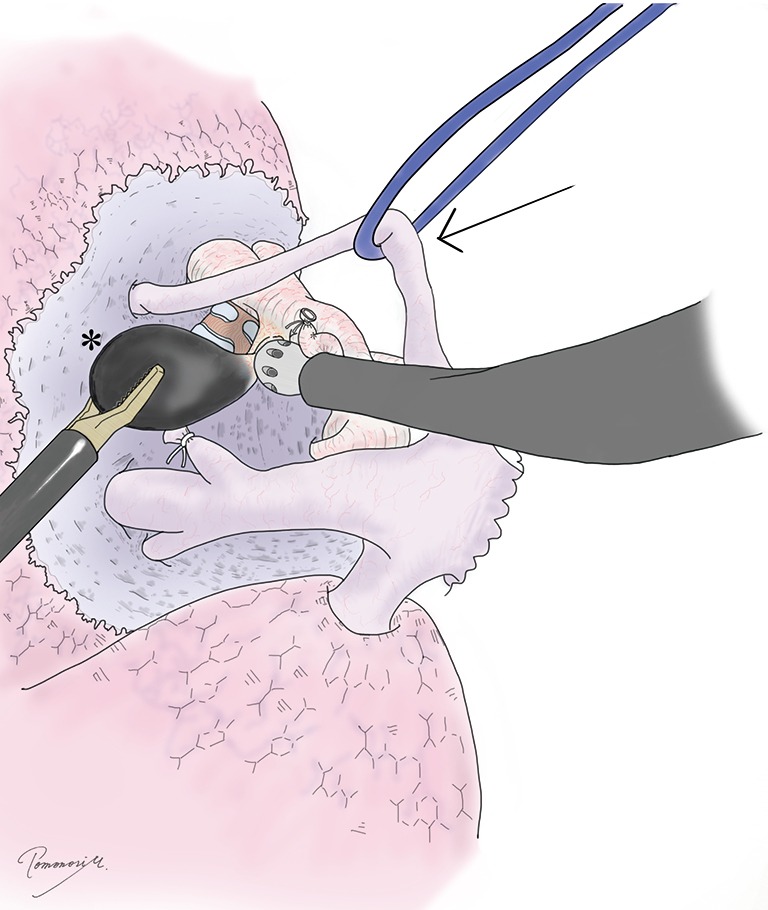
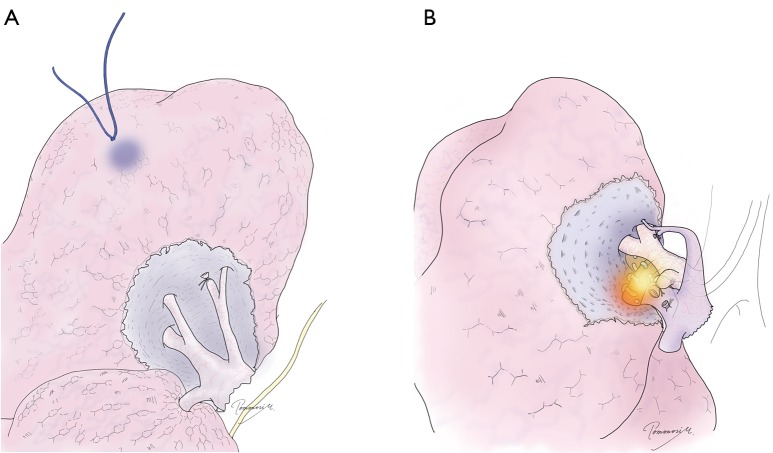
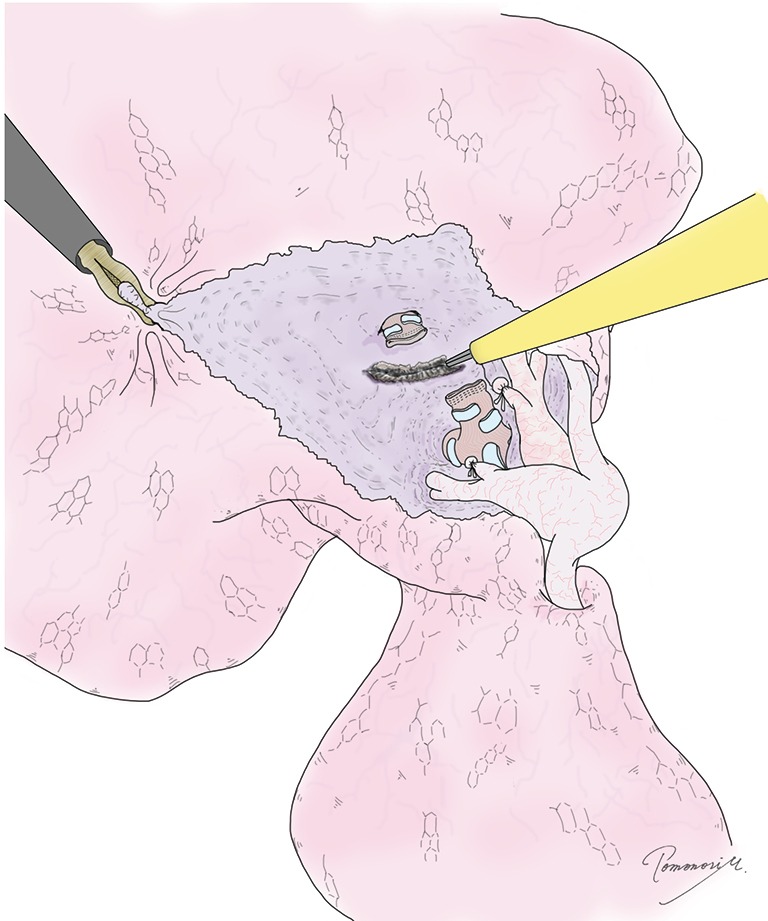
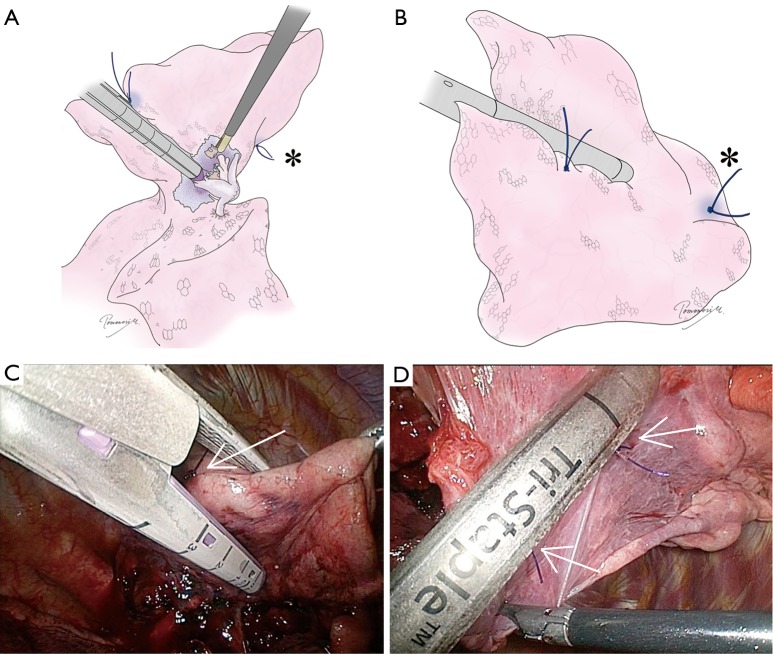
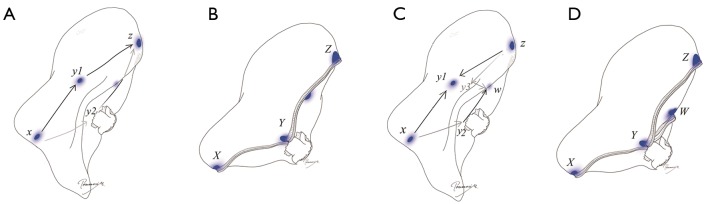
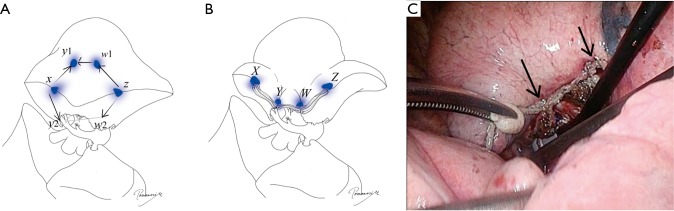
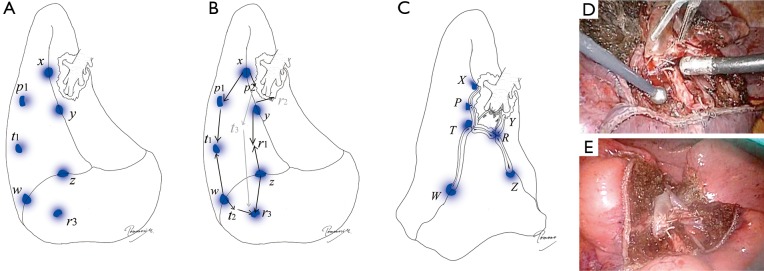
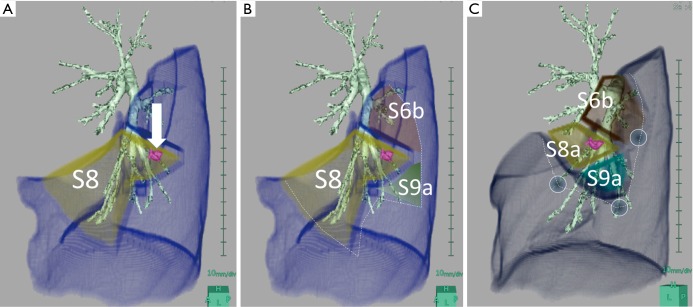
Anatomical segmentectomies play an important role in oncological lung resection, particularly for ground-glass types of primary lung cancers. This operation can also be applied to metastatic lung tumors deep in the lung. Virtual assisted lung mapping (VAL-MAP) is a novel technique that allows for bronchoscopic multi-spot dye markings to provide "geometric information" to the lung surface, using three-dimensional virtual images. In addition to wedge resections, VAL-MAP has been found to be useful in thoracoscopic segmentectomies, particularly complex segmentectomies, such as combined subsegmentectomies or extended segmentectomies. There are five steps in VAL-MAP-assisted segmentectomies: (I) "standing" stitches along the resection lines; (II) cleaning hilar anatomy; (III) confirming hilar anatomy; (IV) going 1 cm deeper; (V) step-by-step stapling technique. Depending on the anatomy, segmentectomies can be classified into linear (lingular, S6, S2), V- or U-shaped (right S1, left S3, S2b + S3a), and three dimensional (S7, S8, S9, S10) segmentectomies. Particularly three dimensional segmentectomies are challenging in the complexity of stapling techniques. This review focuses on how VAL-MAP can be utilized in segmentectomy, and how this technique can assist the stapling process in even the most challenging ones.
Keywords: Lung cancer; bronchoscopy; marking; segmentectomy; video-assisted thoracoscopic surgery (VATS).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Sato M. Virtual assisted lung mapping: navigational thoracoscopic lung resection. Cancer Res Front 2016;2:85-104. 10.17980/2016.85 - DOI
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources