

Optimized Left Ventricular Endocardial Stimulation Is Superior to Optimized Epicardial Stimulation in Ischemic Patients With Poor Response to Cardiac Resynchronization Therapy: A Combined Magnetic Resonance Imaging, Electroanatomic Contact Mapping, and Hemodynamic Study to Target Endocardial Lead Placement
- PMID: 28066827
- PMCID: PMC5196018
- DOI: 10.1016/j.jacep.2016.04.006
Optimized Left Ventricular Endocardial Stimulation Is Superior to Optimized Epicardial Stimulation in Ischemic Patients With Poor Response to Cardiac Resynchronization Therapy: A Combined Magnetic Resonance Imaging, Electroanatomic Contact Mapping, and Hemodynamic Study to Target Endocardial Lead Placement
Abstract
Objectives: The purpose of this study was to identify the optimal pacing site for the left ventricular (LV) lead in ischemic patients with poor response to cardiac resynchronization therapy (CRT).
Background: LV endocardial pacing may offer benefit over conventional CRT in ischemic patients.
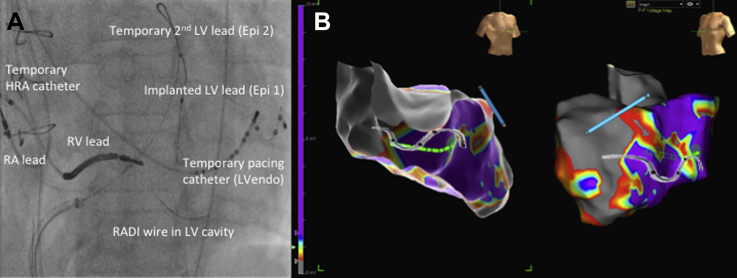
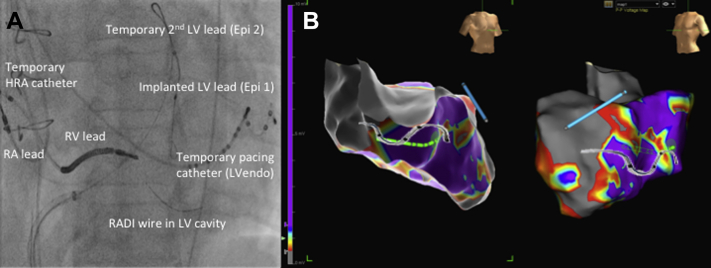
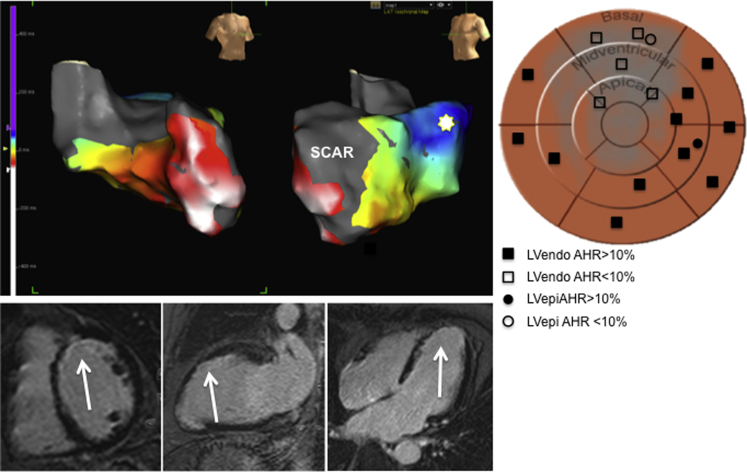
Methods: We performed cardiac magnetic resonance, invasive electroanatomic mapping (EAM), and measured the acute hemodynamic response (AHR) in patients with existing CRT systems.
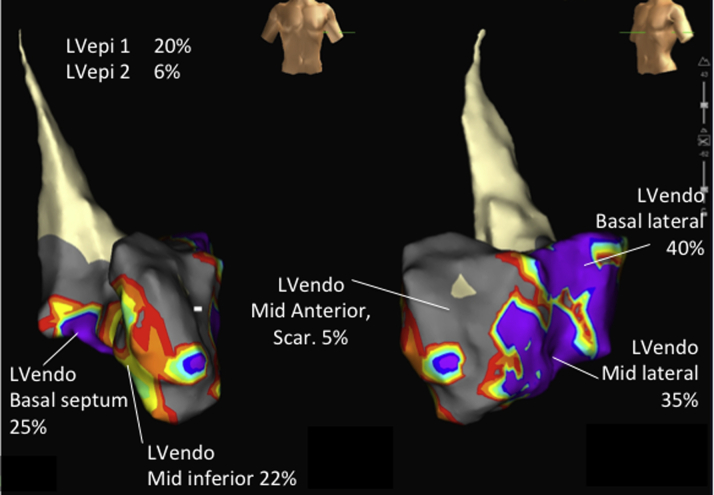
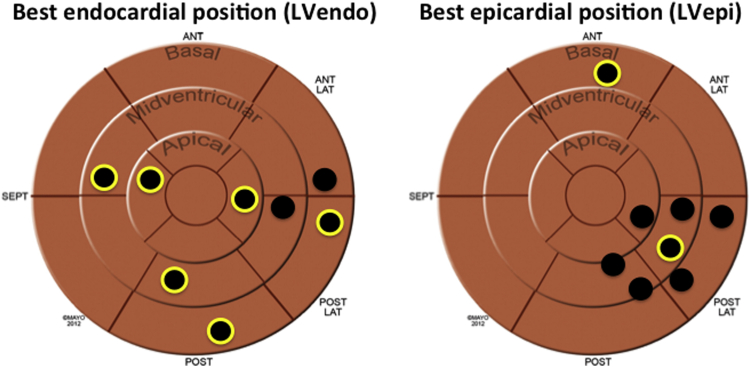
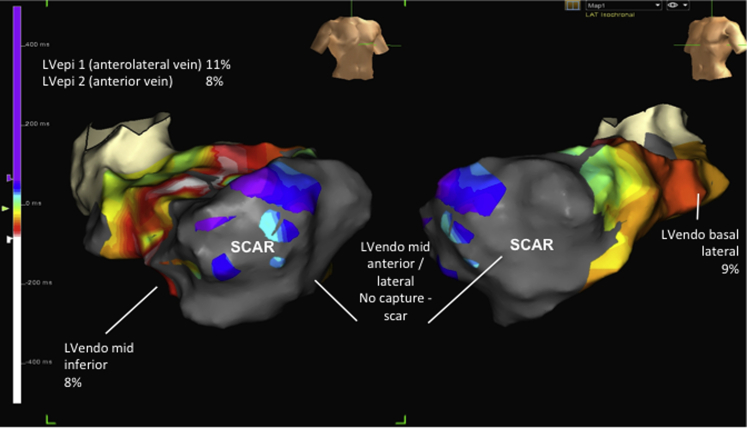
Results: In all, 135 epicardial and endocardial pacing sites were tested in 8 patients. Endocardial pacing was superior to epicardial pacing with respect to mean AHR (% change in dP/dtmax vs. baseline) (11.81 [-7.2 to 44.6] vs. 6.55 [-11.0 to 19.7]; p = 0.025). This was associated with a similar first ventricular depolarization (Q-LV) (75 ms [13 to 161 ms] vs. 75 ms [25 to 129 ms]; p = 0.354), shorter stimulation-QRS duration (15 ms [7 to 43 ms] vs. 19 ms [5 to 66 ms]; p = 0.010) and shorter paced QRS duration (149 ms [95 to 218 ms] vs. 171 ms [120 to 235 ms]; p < 0.001). The mean best achievable AHR was higher with endocardial pacing (25.64 ± 14.74% vs. 12.64 ± 6.76%; p = 0.044). Furthermore, AHR was significantly greater pacing the same site endocardially versus epicardially (15.2 ± 10.7% vs. 7.6 ± 6.3%; p = 0.014) with a shorter paced QRS duration (137 ± 22 ms vs. 166 ± 30 ms; p < 0.001) despite a similar Q-LV (70 ± 38 ms vs. 79 ± 34 ms; p = 0.512). Lack of capture due to areas of scar (corroborated by EAM and cardiac magnetic resonance) was associated with a poor AHR.
Conclusions: In ischemic patients with poor CRT response, biventricular endocardial pacing is superior to epicardial pacing. This may reflect accessibility to sites that cannot be reached via coronary sinus anatomy and/or by access to more rapidly conducting tissue. Furthermore, guidance to the optimal LV pacing site may be aided by modalities such as cardiac magnetic resonance to target delayed activating sites while avoiding scar.
Keywords: AHR, acute hemodynamic response; CMR, cardiac magnetic resonance; CRT; CRT, cardiac resynchronization therapy; EAM, electroanatomic mapping; LV, left ventricle/ventricular; LVendo, left ventricular endocardium; LVepi, optimal epicardial response; LVepi1, implanted LV lead; LVepi2, temporary LV lead; Q-LV, first ventricular depolarization; cardiac magnetic resonance imaging; electroanatomic map; endocardial pacing.
Figures
Comment in
-
Left Ventricular Endocardial Stimulation in Patients With a Poor Response to Cardiac Resynchronization Therapy: What Is Next?JACC Clin Electrophysiol. 2016 Dec;2(7):810-811. doi: 10.1016/j.jacep.2016.06.003. Epub 2016 Aug 3. JACC Clin Electrophysiol. 2016. PMID: 29759764 No abstract available.
References
-
- Cleland J.G.F., Daubert J.-C., Erdmann E. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005;352:1539–1549. - PubMed
-
- Bristow M.R., Saxon L., Boehmer J. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350:2140–2150. - PubMed
-
- Brignole M., Auricchio A., Baron-Esquivias G. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association. Eur Heart J. 2013;34:2281–2329. - PubMed
-
- Daubert J.-C., Saxon L., Adamson P.B. 2012 EHRA/HRS expert consensus statement on cardiac resynchronization therapy in heart failure: implant and follow-up recommendations and management. Europace. 2012;14:1236–1286. - PubMed
-
- Bleeker G.B., Kaandorp T.A., Lamb H.J. Effect of posterolateral scar tissue on clinical and echocardiographic improvement after cardiac resynchronization therapy. Circulation. 2006;113:969–976. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
