

Dialysate Sodium: Rationale for Evolution over Time
- PMID: 28066913
- PMCID: PMC5334180
- DOI: 10.1111/sdi.12570
Dialysate Sodium: Rationale for Evolution over Time
Abstract
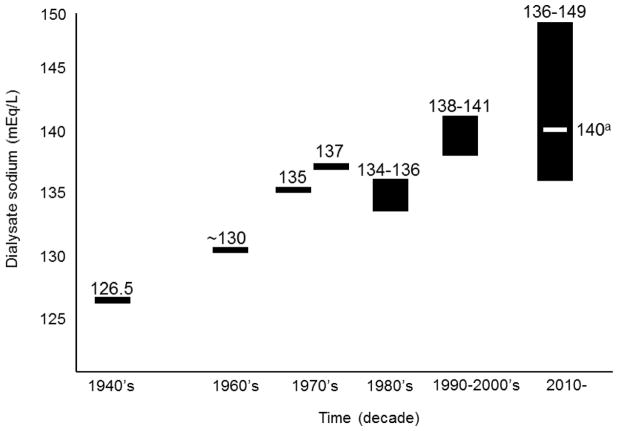
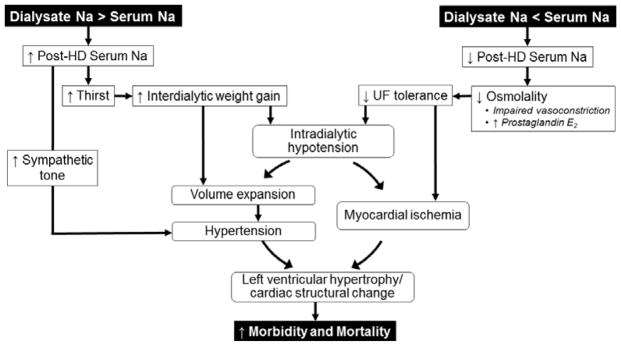
Oligo-anuric individuals receiving hemodialysis (HD) are dependent on the dialysis machine to regulate sodium and water balance. Interest in adjusting the dialysate sodium concentration to promote tolerance of the HD procedure dates back to the early years of dialysis therapy. Evolution of dialysis equipment technologies and clinical characteristics of the dialysis population have prompted clinicians to increase the dialysate sodium concentration over time. Higher dialysate sodium concentrations generally promote hemodynamic stabilization and reduce intradialytic symptoms but often do so at the expense of stimulating thirst and promoting volume expansion. The opposite may be true for lower dialysate sodium concentrations. Observational data suggest that the association between dialysate sodium and outcomes may differ by serum sodium levels, supporting the trend toward individualization of the dialysate sodium prescription. However, lack of randomized controlled clinical trial data, along with operational safety concerns related to individualized dialysate sodium prescriptions, have prevented expert consensus regarding the optimal approach to the dialysate sodium prescription.
© 2017 Wiley Periodicals, Inc.
Figures
References
-
- Peixoto AJ, Gowda N, Parikh CR, Santos SF. Long-term stability of serum sodium in hemodialysis patients. Blood Purif. 2010;29:264–267. - PubMed
-
- Charra B. Fluid balance, dry weight, and blood pressure in dialysis. Hemodial Int. 2007;11:21–31. - PubMed
-
- Scribner BH, Buri R, Caner JE, Hegstrom R, Burnell JM. The treatment of chronic uremia by means of intermittent hemodialysis: a preliminary report. Trans Am Soc Artif Intern Organs. 1960;6:114–122. - PubMed
-
- Drukker W, Parsons FM, Maher JF. Replacement of Renal Function by Dialysis: A Textbook of Dialysis. Boston, MA: Kluwer Boston Inc; 1983.
-
- Sam R, Vaseemuddin M, Leong WH, Rogers BE, Kjellstrand CM, Ing TS. Composition and clinical use of hemodialysates. Hemodial Int. 2006;10:15–28. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
