

Vaginal progesterone decreases preterm birth and neonatal morbidity and mortality in women with a twin gestation and a short cervix: an updated meta-analysis of individual patient data
- PMID: 28067007
- PMCID: PMC5396280
- DOI: 10.1002/uog.17397
Vaginal progesterone decreases preterm birth and neonatal morbidity and mortality in women with a twin gestation and a short cervix: an updated meta-analysis of individual patient data
Abstract
Objective: To assess the efficacy of vaginal progesterone for the prevention of preterm birth and neonatal morbidity and mortality in asymptomatic women with a twin gestation and a sonographic short cervix (cervical length ≤ 25 mm) in the mid-trimester.
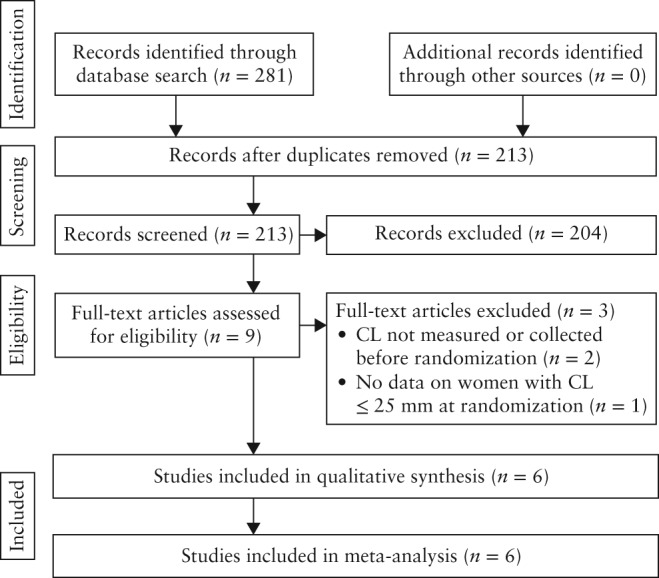
Methods: This was an updated systematic review and meta-analysis of individual patient data (IPD) from randomized controlled trials comparing vaginal progesterone with placebo/no treatment in women with a twin gestation and a mid-trimester sonographic cervical length ≤ 25 mm. MEDLINE, EMBASE, POPLINE, CINAHL and LILACS (all from inception to 31 December 2016), the Cochrane Central Register of Controlled Trials, Research Registers of ongoing trials, Google Scholar, conference proceedings and reference lists of identified studies were searched. The primary outcome measure was preterm birth < 33 weeks' gestation. Two reviewers independently selected studies, assessed the risk of bias and extracted the data. Pooled relative risks (RRs) with 95% confidence intervals (CI) were calculated.
Results: IPD were available for 303 women (159 assigned to vaginal progesterone and 144 assigned to placebo/no treatment) and their 606 fetuses/infants from six randomized controlled trials. One study, which included women with a cervical length between 20 and 25 mm, provided 74% of the total sample size of the IPD meta-analysis. Vaginal progesterone, compared with placebo/no treatment, was associated with a statistically significant reduction in the risk of preterm birth < 33 weeks' gestation (31.4% vs 43.1%; RR, 0.69 (95% CI, 0.51-0.93); moderate-quality evidence). Moreover, vaginal progesterone administration was associated with a significant decrease in the risk of preterm birth < 35, < 34, < 32 and < 30 weeks' gestation (RRs ranging from 0.47 to 0.83), neonatal death (RR, 0.53 (95% CI, 0.35-0.81)), respiratory distress syndrome (RR, 0.70 (95% CI, 0.56-0.89)), composite neonatal morbidity and mortality (RR, 0.61 (95% CI, 0.34-0.98)), use of mechanical ventilation (RR, 0.54 (95% CI, 0.36-0.81)) and birth weight < 1500 g (RR, 0.53 (95% CI, 0.35-0.80)) (all moderate-quality evidence). There were no significant differences in neurodevelopmental outcomes at 4-5 years of age between the vaginal progesterone and placebo groups.
Conclusion: Administration of vaginal progesterone to asymptomatic women with a twin gestation and a sonographic short cervix in the mid-trimester reduces the risk of preterm birth occurring at < 30 to < 35 gestational weeks, neonatal mortality and some measures of neonatal morbidity, without any demonstrable deleterious effects on childhood neurodevelopment. Published 2017. This article is a U.S. Government work and is in the public domain in the USA.
Keywords: cervical length; prematurity; preterm delivery; progestins; progestogens; transvaginal ultrasound.
Published 2017. This article is a U.S. Government work and is in the public domain in the USA.
Figures
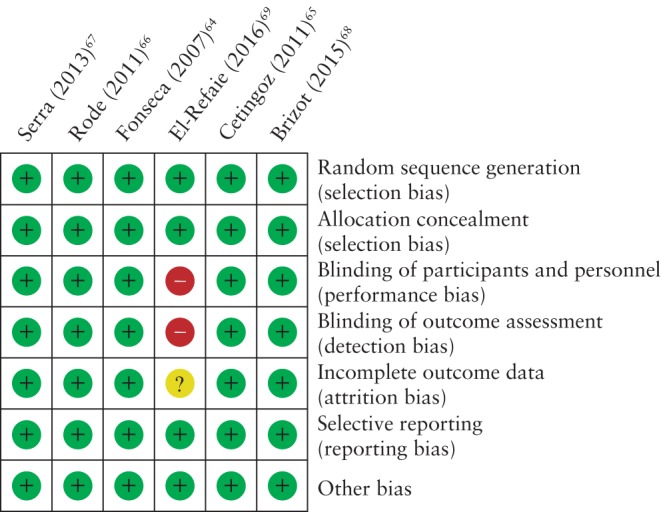
 , low risk of bias;
, low risk of bias;  , high risk of bias;
, high risk of bias;  , unclear risk of bias.
, unclear risk of bias.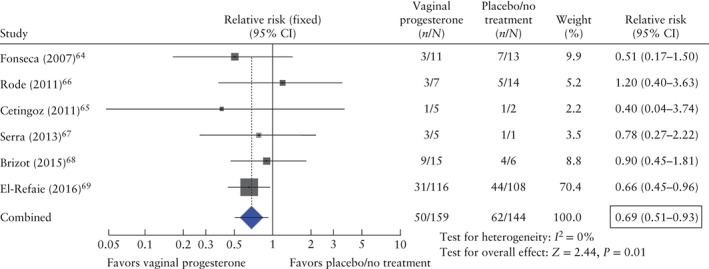
References
-
- Ananth CV, Chauhan SP. Epidemiology of twinning in developed countries. Semin Perinatol 2012; 36: 156–161. - PubMed
-
- Martin JA, Hamilton BE, Osterman MJ. Three decades of twin births in the United States, 1980–2009. NCHS Data Brief 2012; 80: 1–8. - PubMed
-
- Chauhan SP, Scardo JA, Hayes E, Abuhamad AZ, Berghella V. Twins: prevalence, problems, and preterm births. Am J Obstet Gynecol 2010; 203: 305–315. - PubMed
-
- Hamilton BE, Martin JA, Osterman MJ, Curtin SC, Matthews TJ. Births: Final Data for 2014. Natl Vital Stat Rep 2015; 64: 1–64. - PubMed
-
- Conde‐Agudelo A, Belizán JM, Lindmark G. Maternal morbidity and mortality associated with multiple gestations. Obstet Gynecol 2000; 95: 899–904. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
