

Pulmonary fibrosis: tissue characterization using late-enhanced MRI compared with unenhanced anatomic high-resolution CT
- PMID: 28067202
- PMCID: PMC5338575
- DOI: 10.5152/dir.2016.15331
Pulmonary fibrosis: tissue characterization using late-enhanced MRI compared with unenhanced anatomic high-resolution CT
Abstract
Purpose: We aimed to prospectively evaluate anatomic chest computed tomography (CT) with tissue characterization late gadolinium-enhanced magnetic resonance imaging (MRI) in the evaluation of pulmonary fibrosis (PF).
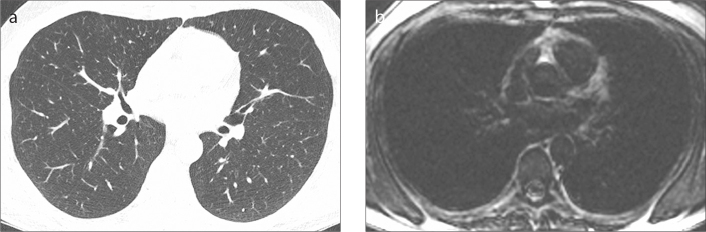
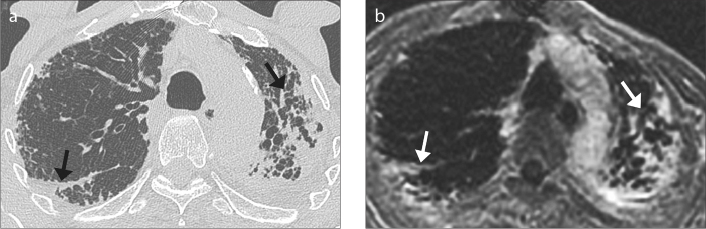
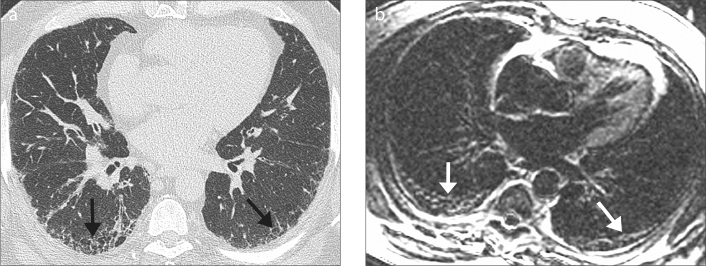
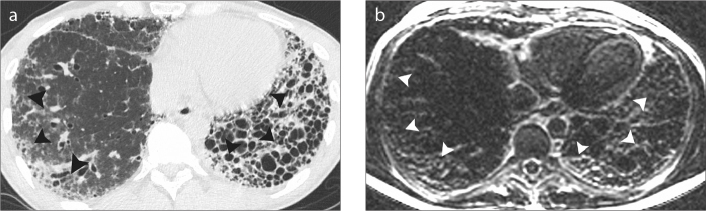
Methods: Twenty patients with idiopathic pulmonary fibrosis (IPF) and twelve control patients underwent late-enhanced MRI and high-resolution CT. Tissue characterization of PF was depicted using a segmented inversion-recovery turbo low-angle shot MRI sequence. Pulmonary arterial blood pool nulling was achieved by nulling main pulmonary artery signal. Images were read in random order by a blinded reader for presence and extent of overall PF (reticulation and honeycombing) at five anatomic levels. Overall extent of IPF was estimated to the nearest 5% as well as an evaluation of the ratios of IPF made up of reticulation and honeycombing. Overall grade of severity was dependent on the extent of reticulation and honeycombing.
Results: No control patient exhibited contrast enhancement on lung late-enhanced MRI. All IPF patients were identified with late-enhanced MRI. Mean signal intensity of the late-enhanced fibrotic lung was 31.8±10.6 vs. 10.5±1.6 for normal lung regions, P < 0.001, resulting in a percent elevation in signal intensity from PF of 204.8%±90.6 compared with the signal intensity of normal lung. The mean contrast-to-noise ratio was 22.8±10.7. Late-enhanced MRI correlated significantly with chest CT for the extent of PF (R=0.78, P = 0.001) but not for reticulation, honeycombing, or coarseness of reticulation or honeycombing.
Conclusion: Tissue characterization of IPF is possible using inversion recovery sequence thoracic MRI.
Conflict of interest statement
The authors declared no conflicts of interest.
Figures
References
-
- Lynch DA, Godwin JD, Safrin S, et al. High-resolution computed tomography in idiopathic pulmonary fibrosis: diagnosis and prognosis. Am J Respir Crit Care Med. 2005;172:488–493. https://doi.org/10.1164/rccm.200412-1756OC. - DOI - PubMed
-
- Raghu G, Collard HR, Egan JJ, et al. An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med. 2011;183:788–824. https://doi.org/10.1164/rccm.2009-040GL. - DOI - PMC - PubMed
-
- Raghu G, Lynch D, Godwin JD, et al. Diagnosis of idiopathic pulmonary fibrosis with high-resolution CT in patients with little or no radiological evidence of honeycombing: secondary analysis of a randomised, controlled trial. Lancet Respir Med. 2014;2:277–284. https://doi.org/10.1016/S2213-2600(14)70011-6. - DOI - PubMed
-
- Raghu G. Idiopathic pulmonary fibrosis: new evidence and an improved standard of care in 2012. Lancet. 2012;380:699–701. https://doi.org/10.1016/S0140-6736(12)61256-2. - DOI - PubMed
-
- Corteville DMR, Kjørstad A, Henzler T, Zöllner FG, Schad LR. Fourier decomposition pulmonary MRI using a variable flip angle balanced steady-state free precession technique. Magn Reson Med. 2015;73:1999–2004. https://doi.org/10.1002/mrm.25293. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
