

Characterisation of the opposing effects of G6PD deficiency on cerebral malaria and severe malarial anaemia
- PMID: 28067620
- PMCID: PMC5222559
- DOI: 10.7554/eLife.15085
Characterisation of the opposing effects of G6PD deficiency on cerebral malaria and severe malarial anaemia
Abstract
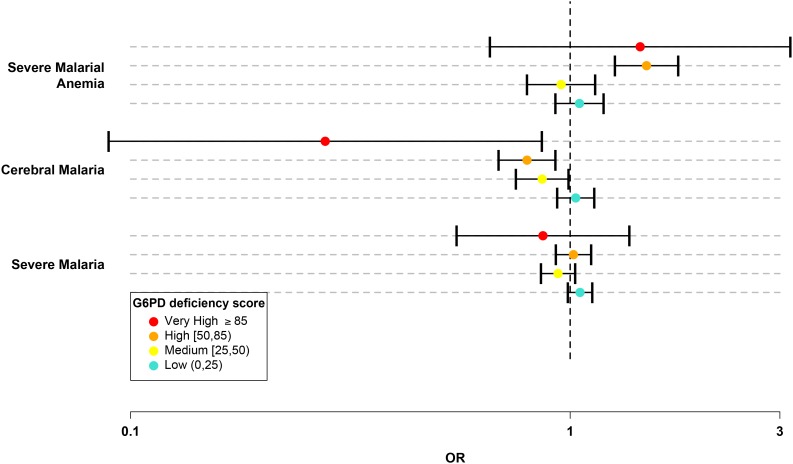
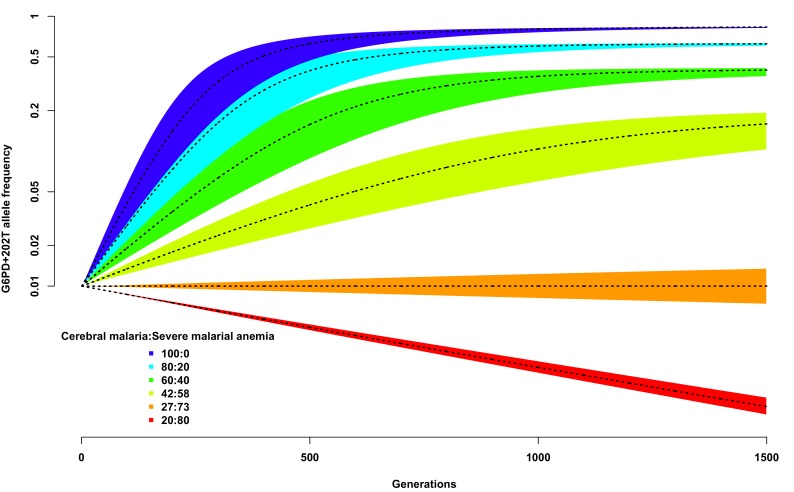
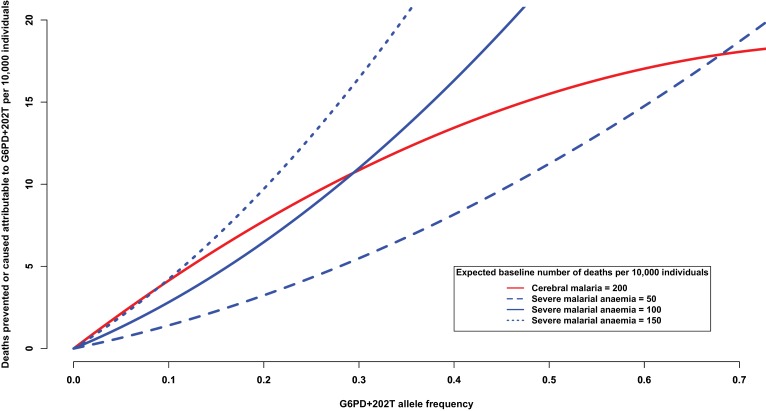
Glucose-6-phosphate dehydrogenase (G6PD) deficiency is believed to confer protection against Plasmodium falciparum malaria, but the precise nature of the protective effecthas proved difficult to define as G6PD deficiency has multiple allelic variants with different effects in males and females, and it has heterogeneous effects on the clinical outcome of P. falciparum infection. Here we report an analysis of multiple allelic forms of G6PD deficiency in a large multi-centre case-control study of severe malaria, using the WHO classification of G6PD mutations to estimate each individual's level of enzyme activity from their genotype. Aggregated across all genotypes, we find that increasing levels of G6PD deficiency are associated with decreasing risk of cerebral malaria, but with increased risk of severe malarial anaemia. Models of balancing selection based on these findings indicate that an evolutionary trade-off between different clinical outcomes of P. falciparum infection could have been a major cause of the high levels of G6PD polymorphism seen in human populations.
Keywords: G6PD deficiency; epidemiology; evolutionary biology; genetic association; genomics; global health; human; infectious disease; selection.
Conflict of interest statement
JF: Director of the Wellcome Trust, one of the three founding funders of eLife. The other authors declare that no competing interests exist.
Figures
References
-
- Beutler E. G6PD deficiency. Blood. 1994;84:3613–3636. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
