

ACUTE CENTRAL SEROUS CHORIORETINOPATHY: Factors Influencing Episode Duration
- PMID: 28067724
- PMCID: PMC5642321
- DOI: 10.1097/IAE.0000000000001443
ACUTE CENTRAL SEROUS CHORIORETINOPATHY: Factors Influencing Episode Duration
Abstract
Purpose: To evaluate the influence of clinical and multimodal imaging parameters on the duration of acute central serous chorioretinopathy (CSCR) episodes.
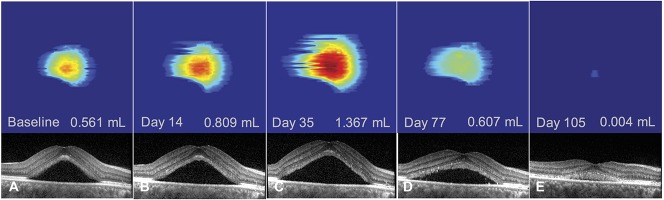
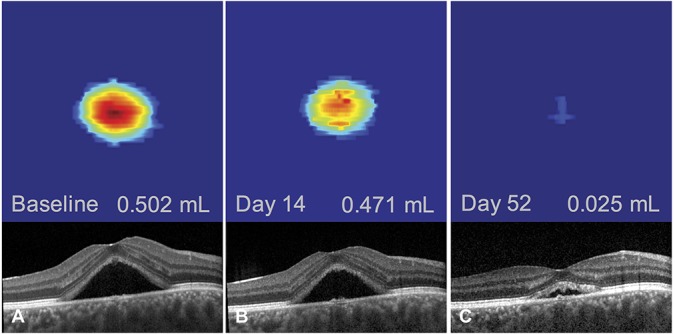
Methods: Consecutive patients with first, treatment-naïve central serous chorioretinopathy episodes presenting within 20 days of symptoms onset were prospectively included. They were reevaluated 15 days to 20 days later, followed by monthly evaluation for 6 months. Subfoveal choroidal thickness (SFCT), fluorescein leakage intensity on fluorescein angiography, elevation of retinal pigment epithelium (RPE) lesions at leakage sites, focal/multifocal pattern of indocyanine green angiography (ICGA) at baseline, time-dependent pattern of subretinal fluid (SRF) resorption on OCT using volume segmentation, history of corticosteroid intake and mean blood pressure were evaluated using univariate (Log rank test) and multivariate (Cox proportional hazard regression) survival analysis.
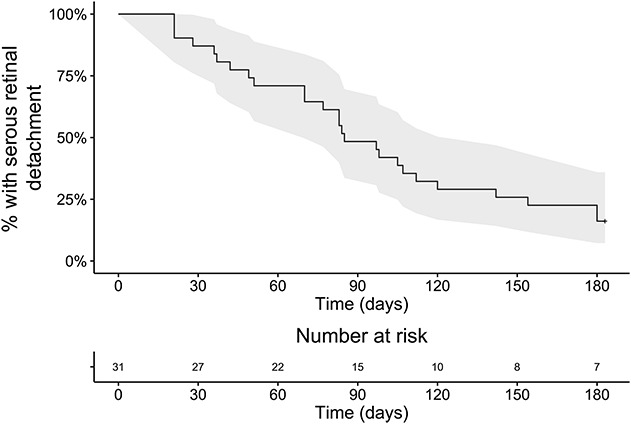
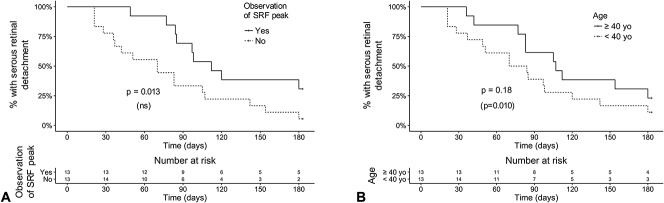
Results: Thirty-one patients were included (26 men, 5 women, mean age: 40.0 ± 8.9 years, range: 24-58), of which 26 (84%) had episode resolution by 6 months. Using univariate analysis, episode duration was longer in cases with subfoveal choroidal thickness ≥500 μm (P = 0.0002), retinal pigment epithelium elevation at leakage sites ≥50 μm (P = 0.033), and a peak in subretinal fluid observed during follow-up (P = 0.013), and there was a near-significant association of intense fluorescein leakage (P = 0.074) with longer episodes. Using multivariate analysis, subfoveal choroidal thickness ≥500 μm (P = 0.017), retinal pigment epithelium elevation at leakage sites ≥50 μm (P = 0.010) and patient age ≥40 years (P = 0.010) were significantly and independently associated to longer episodes. Indocyanine green angiography pattern, corticosteroid intake, and blood pressure did not influence episode duration.
Conclusion: Older age, higher subfoveal choroidal thickness, and higher degree of retinal pigment epithelium alteration at leakage sites are independent factors of longer acute central serous chorioretinopathy episodes.
Conflict of interest statement
None of the authors has any financial/conflicting interests to disclose.
Figures

References
-
- Klein ML, Van Buskirk EM, Friedman E, et al. Experience with nontreatment of central serous choroidopathy. Arch Ophthalmol 1974;91:247–250. - PubMed
-
- Robertson DM, Ilstrup D. Direct, indirect, and sham laser photocoagulation in the management of central serous chorioretinopathy. Am J Ophthalmol 1983;95:457–466. - PubMed
-
- Daruich A, Matet A, Dirani A, et al. Central serous chorioretinopathy: recent findings and new physiopathology hypothesis. Prog Retin Eye Res 2015;48:82–118. - PubMed
-
- Malik KJ, Sampat KM, Mansouri A, et al. Low-intensity/high-density subthreshold micropulse diode laser for chronic central serous chorioretinopathy. Retina 2015;35:532–536. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
