

A simple scoring model for advanced colorectal neoplasm in asymptomatic subjects aged 40-49 years
- PMID: 28068908
- PMCID: PMC5223374
- DOI: 10.1186/s12876-016-0562-9
A simple scoring model for advanced colorectal neoplasm in asymptomatic subjects aged 40-49 years
Abstract
Background: Limited data are available for advanced colorectal neoplasm in asymptomatic individuals aged 40-49 years. We aimed to identify risk factors and develop a simple prediction model for advanced colorectal neoplasm in these persons.
Methods: Clinical data were collected on 2781 asymptomatic subjects aged 40-49 years who underwent colonoscopy for routine health examination. Subjects were randomly allocated to a development or validation set. Logistic regression analysis was used to determine predictors of advanced colorectal neoplasm.
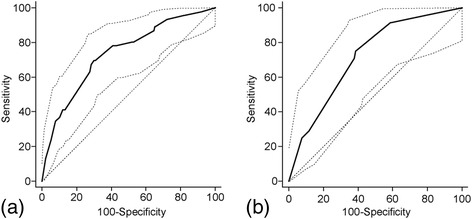
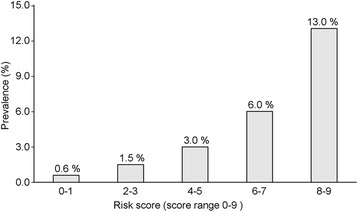
Results: The prevalence of overall and advanced colorectal neoplasm was 20.2 and 2.5% respectively. Older age (45-49 years), male sex, positive serology of Helicobacter pylori, and high triglyceride and low high-density lipoprotein (HDL) levels were independently associated with an increased risk of advanced colorectal neoplasm. BMI (body mass index) was not significant in multivariable analysis. We developed a simple scoring model for advanced colorectal neoplasm (range 0-9). A cutoff of ≥4 defined 43% of subjects as high risk for advanced colorectal neoplasm (sensitivity, 79%; specificity, 58%; area under the receiver operating curve = 0.72) in the validation datasets.
Conclusion: Older age (45-49 years), male sex, positive serology of H. pylori, high triglyceride level, and low HDL level were identified as independent risk factors for advanced colorectal neoplasm.
Keywords: Adenoma; Colonoscopy; Colorectal neoplasm; Risk assessment; Screening.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
