

Preoperative predictors for early recurrence of resectable pancreatic cancer
- PMID: 28069033
- PMCID: PMC5223494
- DOI: 10.1186/s12957-016-1078-z
Preoperative predictors for early recurrence of resectable pancreatic cancer
Abstract
Background: The first-line treatment for resectable pancreatic cancer (RPC) is surgical resection. However, our patients have often experienced early recurrence after curative resection for RPC, with desperately poor prognosis. Some reports indicated that minimally distant metastasis not detected at operation might cause early recurrence. The present study aimed to identify preoperative clinicopathological features of early recurrence after curative resection of RPC.
Methods: Ninety RPC patients who underwent curative resection between 2000 and 2014 at our institution were retrospectively analyzed.
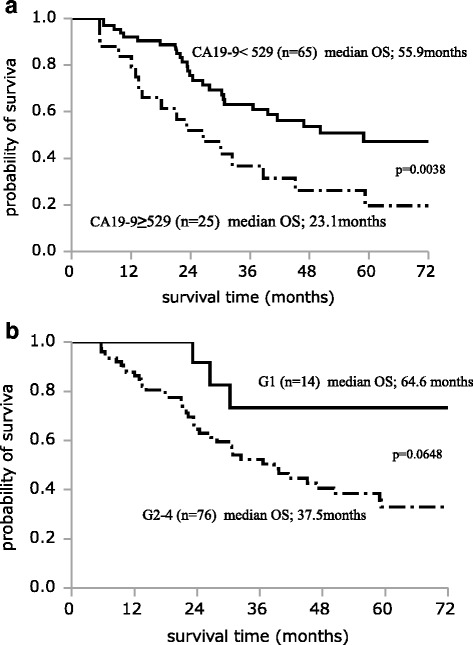
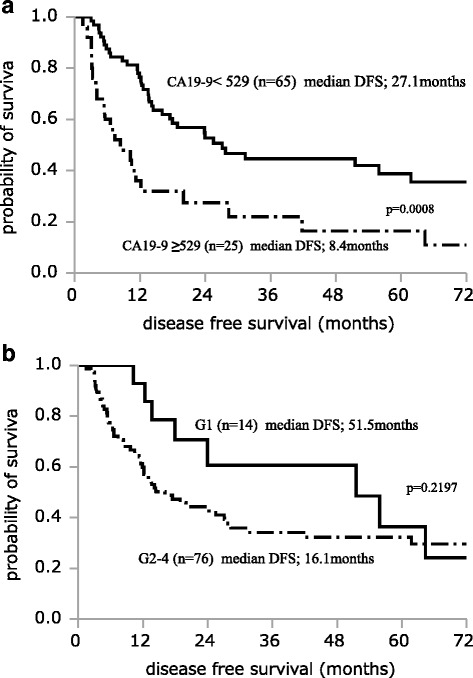
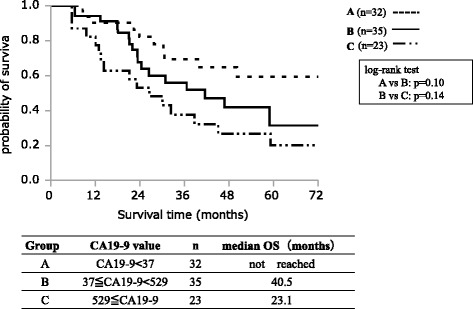
Results: Of the 90 patients, 32 had recurrence within 1 year. Univariate analysis demonstrated that preoperative serum carbohydrate antigen (CA19-9) ≥529 U/mL (P = 0.0011), preoperative serum s-pancreas-1 antigen (SPan-1) ≥37 U/mL (P = 0.0038), and histological grades G2-G4 (P = 0.0158) were significantly associated with recurrence within 1 year after curative resection. Multivariate analysis demonstrated that preoperative serum CA19-9 ≥ 529 U/mL (P = 0.0477) and histological grade G2-G4 (P = 0.0129) were independent predictors of recurrence within 1 year. Recurrent cases within 1 year postoperatively had significantly more distant metastasis than cases with no recurrence within 1 year (P < 0.001).
Conclusions: Preoperative serum CA19-9 ≥ 529 U/mL and histological grades G2-G4 were independent predictive factors for recurrence within 1 year after pancreatectomy for RPC. Furthermore, recurrent cases within 1 year had more frequent distant metastasis than cases with no recurrence within 1 year. These results suggest that RPC patients with preoperative serum CA19-9 ≥ 529 U/mL should receive preoperative therapy rather than surgery.
Keywords: CA19-9; Histological grade; Preoperative predictors; Resectable pancreatic cancer; Tumor diameter.
Figures
References
-
- Kimura K, Amano R, Nakata B, Yamazoe S, Hirata K, Murata A, Miura K, Nishio K, Hirakawa T, Ohira M, Hirakawa K. Clinical and pathological features of five-year survivors after pancreatectomy for pancreatic adenocarcinoma. World J Surg Oncol. 2014;12:360. doi: 10.1186/1477-7819-12-360. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
