

Optimal configuration of adhesive ECG patches suitable for long-term monitoring of a vectorcardiogram
- PMID: 28069275
- PMCID: PMC5420469
- DOI: 10.1016/j.jelectrocard.2016.12.005
Optimal configuration of adhesive ECG patches suitable for long-term monitoring of a vectorcardiogram
Abstract
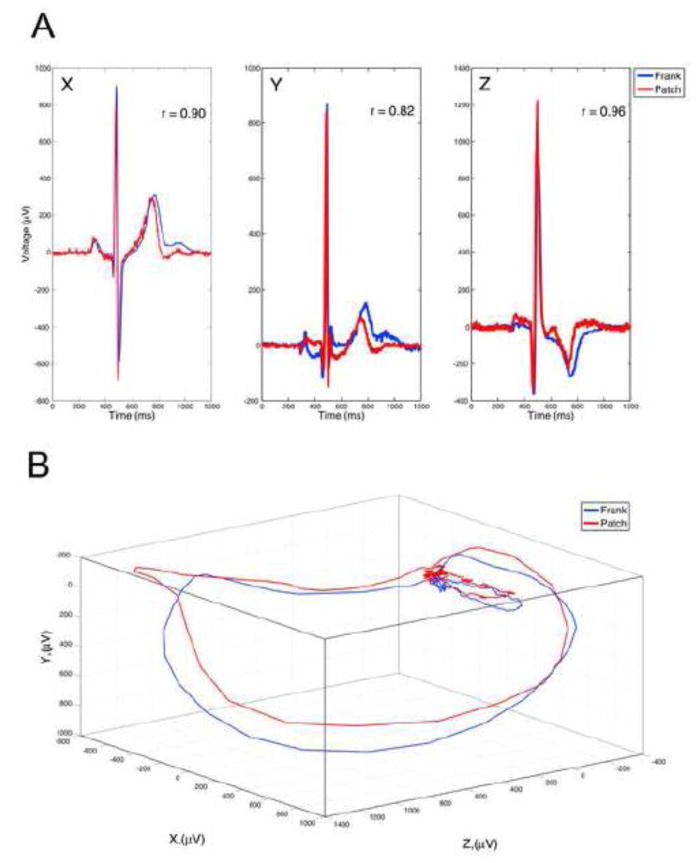
The purpose of this study was to develop optimal configuration of adhesive ECG patches placement on the torso, which would provide the best agreement with the Frank orthogonal ECGs. Ten seconds of orthogonal ECG followed by 3-5min of ECGs using patches at 5 different locations simultaneously on the torso were recorded in 50 participants at rest in sitting position. Median beat was generated for each ECG and 3 patch ECGs that best correlate with orthogonal ECGs were selected for each participant. For agreement analysis, spatial QRS-T angle, spatial QRS and T vector characteristics, spatial ventricular gradient, roundness, thickness and planarity of vectorcardiographic (VCG) loops were measured. Key VCG parameters showed high agreement in Bland-Altman analysis (spatial QRS-T angle on 3-patch ECG vs. Frank ECG bias 0.3 (95% limits of agreement [-6.23;5.71 degrees]), Lin's concordance coefficient=0.996). In conclusion, newly developed orthogonal 3-patch ECG can be used for long-term VCG monitoring.
Keywords: ECG patch; QRS-T angle; Vectorcardiogram.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures

Similar articles
-
The spatial QRS-T angle in the Frank vectorcardiogram: accuracy of estimates derived from the 12-lead electrocardiogram.J Electrocardiol. 2010 Jul-Aug;43(4):294-301. doi: 10.1016/j.jelectrocard.2010.03.009. Epub 2010 Apr 24. J Electrocardiol. 2010. PMID: 20417936
-
The synthesized vectorcardiogram resembles the measured vectorcardiogram in patients with dyssynchronous heart failure.J Electrocardiol. 2015 Jul-Aug;48(4):586-92. doi: 10.1016/j.jelectrocard.2015.04.001. Epub 2015 Apr 8. J Electrocardiol. 2015. PMID: 25900820
-
Comparison of the spatial QRS-T angle derived from digital ECGs recorded using conventional electrode placement with that derived from Mason-Likar electrode position.J Electrocardiol. 2016 Sep-Oct;49(5):714-9. doi: 10.1016/j.jelectrocard.2016.06.006. Epub 2016 Jun 21. J Electrocardiol. 2016. PMID: 27395365
-
A review of beat-to-beat vectorcardiographic (VCG) parameters for analyzing repolarization variability in ECG signals.Biomed Tech (Berl). 2016 Feb;61(1):3-17. doi: 10.1515/bmt-2015-0005. Biomed Tech (Berl). 2016. PMID: 25992510 Review.
-
Vectorcardiographic diagnostic & prognostic information derived from the 12-lead electrocardiogram: Historical review and clinical perspective.J Electrocardiol. 2015 Jul-Aug;48(4):463-75. doi: 10.1016/j.jelectrocard.2015.05.002. Epub 2015 May 8. J Electrocardiol. 2015. PMID: 26027545 Review.
Cited by
-
Wearable sensors for monitoring the internal and external workload of the athlete.NPJ Digit Med. 2019 Jul 29;2:71. doi: 10.1038/s41746-019-0149-2. eCollection 2019. NPJ Digit Med. 2019. PMID: 31372506 Free PMC article. Review.
-
Vectorcardiogram in athletes: The Sun Valley Ski Study.Ann Noninvasive Electrocardiol. 2019 May;24(3):e12614. doi: 10.1111/anec.12614. Epub 2018 Nov 7. Ann Noninvasive Electrocardiol. 2019. PMID: 30403442 Free PMC article.
-
A Pivotal Study to Validate the Performance of a Novel Wearable Sensor and System for Biometric Monitoring in Clinical and Remote Environments.Digit Biomark. 2019 Mar 1;3(1):1-13. doi: 10.1159/000493642. eCollection 2019 Jan-Apr. Digit Biomark. 2019. PMID: 32095764 Free PMC article.
-
A Survey of Challenges and Opportunities in Sensing and Analytics for Risk Factors of Cardiovascular Disorders.ACM Trans Comput Healthc. 2021 Jan;2(1):9. doi: 10.1145/3417958. Epub 2020 Dec 30. ACM Trans Comput Healthc. 2021. PMID: 34337602 Free PMC article.
-
Global ECG Measures and Cardiac Structure and Function: The ARIC Study (Atherosclerosis Risk in Communities).Circ Arrhythm Electrophysiol. 2018 Mar;11(3):e005961. doi: 10.1161/CIRCEP.117.005961. Circ Arrhythm Electrophysiol. 2018. PMID: 29496680 Free PMC article.
References
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. A Report From the American Heart Association. 2015. Heart Disease and Stroke Statistics—2016 Update. - PubMed
-
- Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. Jama. 2001;285:2370–5. - PubMed
-
- Gladstone DJ, Spring M, Dorian P, Panzov V, Thorpe KE, Hall J, et al. Atrial Fibrillation in Patients with Cryptogenic Stroke. New England Journal of Medicine. 2014;370:2467–77. - PubMed
-
- Turakhia MP, Hoang DD, Zimetbaum P, Miller JD, Froelicher VF, Kumar UN, et al. Diagnostic utility of a novel leadless arrhythmia monitoring device. Am J Cardiol. 2013;112:520–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
