

Emergency Department Visits Without Hospitalization Are Associated With Functional Decline in Older Persons
- PMID: 28069299
- PMCID: PMC5365369
- DOI: 10.1016/j.annemergmed.2016.09.018
Emergency Department Visits Without Hospitalization Are Associated With Functional Decline in Older Persons
Abstract
Study objective: Among older persons, disability and functional decline are associated with increased mortality, institutionalization, and costs. The aim of the study was to determine whether illnesses and injuries leading to an emergency department (ED) visit but not hospitalization are associated with functional decline among community-living older persons.
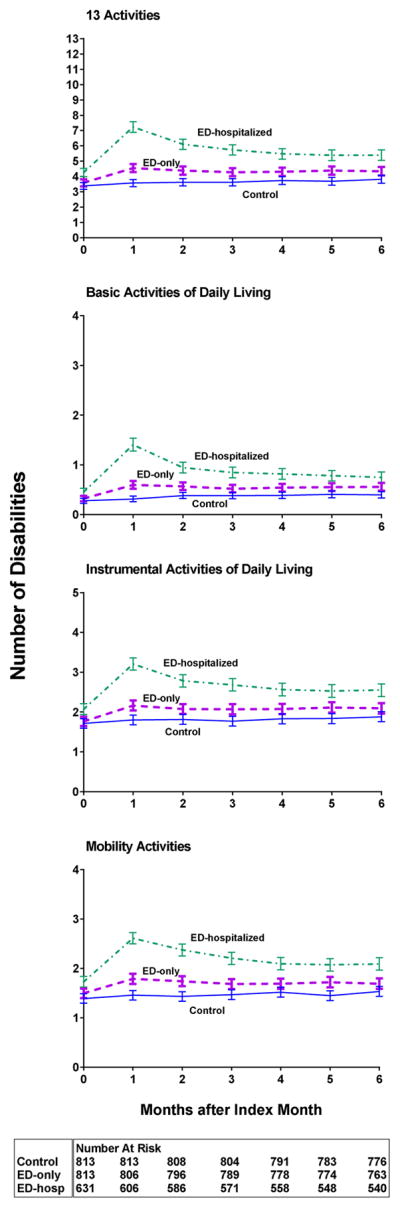
Methods: From a cohort of 754 community-living older persons who have been followed with monthly interviews for up to 14 years, we matched 813 ED visits without hospitalization (ED only) to 813 observations without an ED visit or hospitalization (control). We compared the course of disability during the following 6 months between the 2 matched groups. To establish a frame of reference, we also compared the ED-only group with an unmatched group who were hospitalized after an ED visit (ED-hospitalized). Disability scores (range 0 [lowest] to 13 [highest]) were compared using generalized linear models adjusted for relevant covariates. Admission to a nursing home and mortality were evaluated as secondary outcomes.
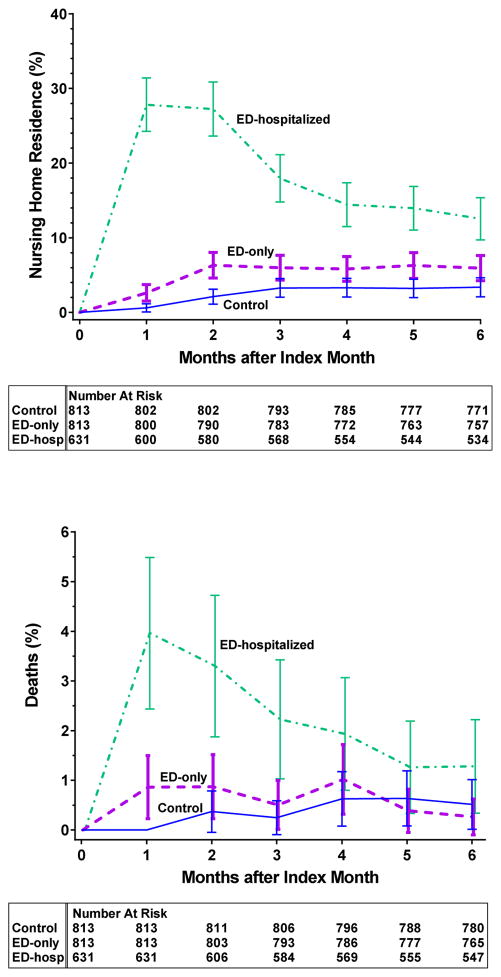
Results: The ED-only and control groups were well matched. For both groups, the mean age was 84 years, and 69% were women. The baseline disability scores were 3.4 and 3.6 in the ED-only and control groups, respectively. During the 6-month follow-up period, the ED-only group had significantly higher disability scores than the control group, with an adjusted risk ratio of 1.14 (95% confidence interval [CI] 1.09 to 1.19). Compared with participants in the ED-only group, those who were hospitalized after an ED visit had disability scores that were significantly higher (risk ratio 1.17; 95% CI 1.12 to 1.22). Both nursing home admissions (hazard ratio 3.11; 95% CI 2.05 to 4.72) and mortality (hazard ratio 1.93; 95% CI 1.07 to 3.49) were higher in the ED-only group versus control group during the 6-month follow-up period.
Conclusion: Although not as debilitating as an acute hospitalization, illnesses and injuries leading to an ED visit without hospitalization were associated with a clinically meaningful decline in functional status during the following 6 months, suggesting that the period after an ED visit represents a vulnerable time for community-living older persons.
Copyright © 2016 American College of Emergency Physicians. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Bending the Curve of Health Trajectories for Older Adults Discharged From the Emergency Department.Ann Emerg Med. 2017 Apr;69(4):434-436. doi: 10.1016/j.annemergmed.2016.10.030. Epub 2016 Dec 29. Ann Emerg Med. 2017. PMID: 28041824 No abstract available.
-
Defining Quality and Outcome in Geriatric Emergency Care.Ann Emerg Med. 2017 Jul;70(1):107-109. doi: 10.1016/j.annemergmed.2017.03.003. Ann Emerg Med. 2017. PMID: 28645389 No abstract available.
References
-
- National Hospital Ambulatory Medical Care Survey: 2010 Emergency Department Summary Tables. Table 2. http://www.cdc.gov/nchs/data/ahcd/nhamcs_emergency/2010_ed_web_tables.pdf.
-
- Aminzadeh F, Dalziel WB. Older adults in the emergency department: a systematic review of patterns of use, adverse outcomes, and effectiveness of interventions. Ann Emerg Med. 2002;39(3):238–247. - PubMed
-
- Fried LP, Guralnik JM. Disability in older adults: evidence regarding significance, etiology, and risk. J Am Geriatr Soc. 1997;45(1):92–100. - PubMed
-
- Chan L, Beaver S, Maclehose RF, Jha A, Maciejewski M, Doctor JN. Disability and health care costs in the Medicare population. Arch Phys Med Rehabil. 2002;83(9):1196–1201. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
