

The HCV Treatment Revolution Continues: Resistance Considerations, Pangenotypic Efficacy, and Advances in Challenging Populations
- PMID: 28070174
- PMCID: PMC5210027
The HCV Treatment Revolution Continues: Resistance Considerations, Pangenotypic Efficacy, and Advances in Challenging Populations
Abstract
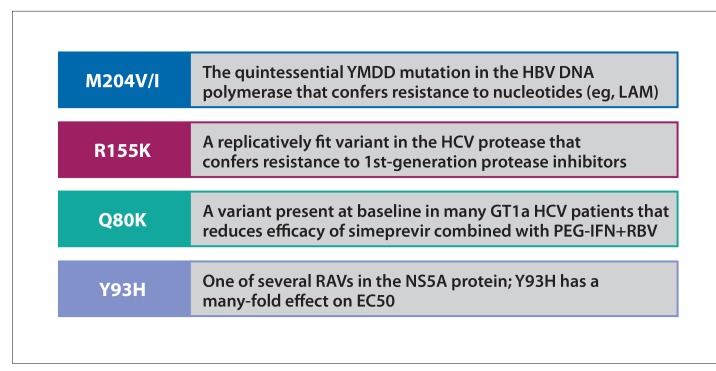
The US Food and Drug Administration has now approved 10 direct-acting antivirals (DAAs) for the management of hepatitis C virus (HCV). These therapies are combined into 6 regimens that are given for varying durations, with or without ribavirin, depending on the viral genotype, the presence or absence of baseline resistance-associated variants (RAVs), and the patient type. RAVs may be present before exposure to a drug or may become detectable de novo during exposure to a drug. Emerging resistant strains are the most common cause of failure of HCV DAA regimens. Second-generation DAAs provide superior coverage of resistant variants compared with first-generation members of that class. They may also cover a broader range of viral genotypes. Numerous clinical trials have evaluated the safety and efficacy of DAAs in a variety of patient populations, including those with cirrhosis, HIV, and end-stage renal disease. This article evaluates the data from these studies, and discusses recommendations from the American Association for the Study of Liver Diseases (AASLD) and the Infectious Diseases Society of America (IDSA) guidance document.
Figures
References
-
- HCV guidance: recommendations for testing, managing, and treating hepatitis C. American Association for the Study of Liver Diseases/Infectious Diseases Society of America. [Accessed September 16, 2016]. http://www.hcvguidelines.org Updated September 16, 2016.
-
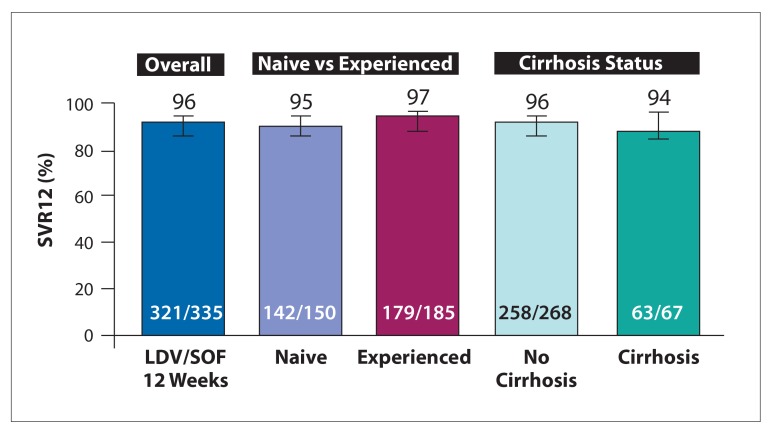
- Afdhal N, Zeuzem S, Kwo P, et al. ION-1 Investigators. Ledipasvir and sofosbuvir for untreated HCV genotype 1 infection. N Engl J Med. 2014;370(20):1889–1898. - PubMed
-
- Afdhal N, Reddy KR, Nelson DR, et al. ION-2 Investigators. Ledipasvir and sofosbuvir for previously treated HCV genotype 1 infection. N Engl J Med. 2014;370(20):1483–1493. - PubMed
-
- Kowdley KV, Gordon SC, Reddy KR, et al. ION-3 Investigators. Ledipasvir and sofosbuvir for 8 or 12 weeks for chronic HCV without cirrhosis. N Engl J Med. 2014;370(20):1879–1888. - PubMed
-
- Zeuzem S, Mizokami M, Pianko S, et al. Prevalence of pre-treatment NS5A resistance associated variants in genotype 1 patients across different regions using deep sequencing and effect on treatment outcome with LDV/SOF [AASLD Meeting Abstract 91] Hepatology. 2015;62(suppl 1)
LinkOut - more resources
Full Text Sources
Other Literature Sources