

Three-dimensional surgical simulation improves the planning for correction of facial prognathism and asymmetry: A qualitative and quantitative study
- PMID: 28071714
- PMCID: PMC5223192
- DOI: 10.1038/srep40423
Three-dimensional surgical simulation improves the planning for correction of facial prognathism and asymmetry: A qualitative and quantitative study
Abstract
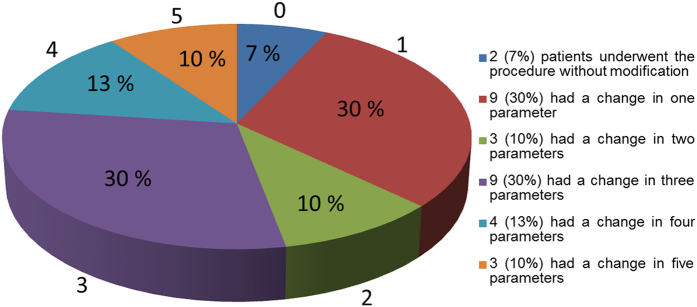
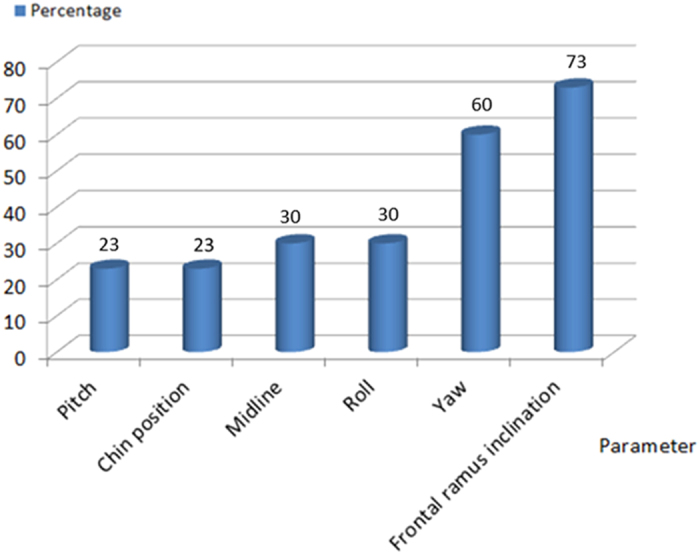
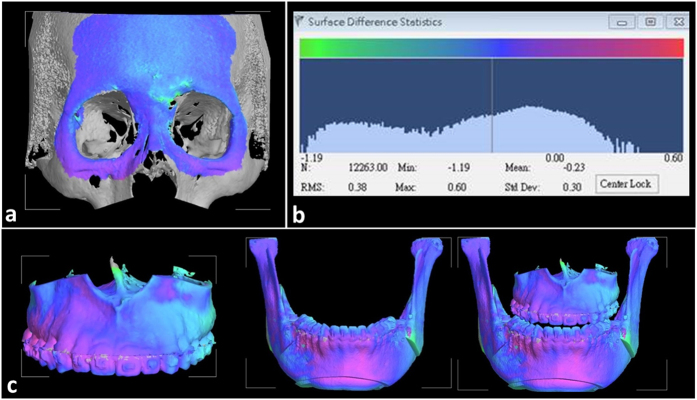
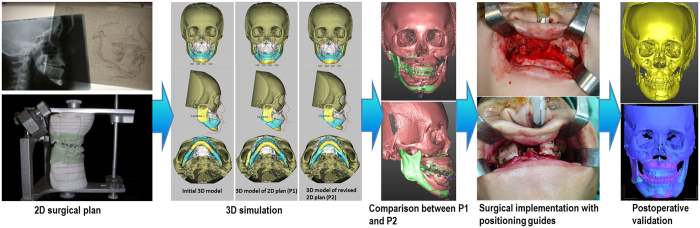
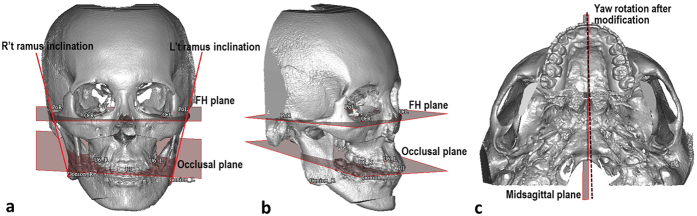
Traditional planning method for orthognathic surgery has limitations of cephalometric analysis, especially for patients with asymmetry. The aim of this study was to assess surgical plan modification after 3-demensional (3D) simulation. The procedures were to perform traditional surgical planning, construction of 3D model for the initial surgical plan (P1), 3D model of altered surgical plan after simulation (P2), comparison between P1 and P2 models, surgical execution, and postoperative validation using superimposition and root-mean-square difference (RMSD) between postoperative 3D image and P2 simulation model. Surgical plan was modified after 3D simulation in 93% of the cases. Absolute linear changes of landmarks in mediolateral direction (x-axis) were significant and between 1.11 to 1.62 mm. The pitch, yaw, and roll rotation as well as ramus inclination correction also showed significant changes after the 3D planning. Yaw rotation of the maxillomandibular complex (1.88 ± 0.32°) and change of ramus inclination (3.37 ± 3.21°) were most frequently performed for correction of the facial asymmetry. Errors between the postsurgical image and 3D simulation were acceptable, with RMSD 0.63 ± 0.25 mm for the maxilla and 0.85 ± 0.41 mm for the mandible. The information from this study could be used to augment the clinical planning and surgical execution when a conventional approach is applied.
Figures
References
-
- Segner D. In Orthodontic Cephalometry (ed. Athanasiou Athanasios E.) (Mosby-Wolfe, London, 1995).
-
- Alexander J. & Richard L. J. In Radiographic Cephalometry from basics to 3-D imaging 2nd edn (eds. Alexander J. & Richard L. J.) (Quintessence Publishing Co, Inc; 2006).
-
- Trpkova B. et al. Assessment of facial asymmetries from posteroanterior cephalograms: Validity of reference lines. Am J Orthod Dentofac Orthop. 123, 512–520 (2003). - PubMed
-
- Ellis E. III. A method to passively align the saggital ramus osteotomy segments. J Oral Maxillofac Surg. 65, 2125–2130 (2007). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
